The nurse assesses a 1-day-old newborn. Which finding indicates that the newborn's oxygenation needs are not being met?
Select one:
Grunting and nasal flaring.
Acrocyanosis.
Abdominal breathing.
Respiratory rate of 54 breaths/minute.
The Correct Answer is A
Choice A Reason: Grunting and nasal flaring. These are signs of respiratory distress in newborns, which indicate that their oxygenation needs are not being met. Grunting and nasal flaring. This is because grunting and nasal flaring are signs of respiratory distress in newborns, which indicate inadequate oxygenation and ventilation. Grunting is a noise made by the newborn when exhaling, which reflects an atempt to keep the alveoli open and increase lung volume.
Nasal flaring is a widening of the nostrils when inhaling, which reflects an effort to reduce airway resistance and increase airflow.
Choice B Reason: Acrocyanosis. This is not a sign of respiratory distress in newborns, but rather a common condition called acrocyanosis. Acrocyanosis means bluish discoloration of the hands and feet due to poor peripheral circulation in response to cold exposure or stress. It does not affect oxygenation or ventilation and usually disappears within 24 to 48 hours after birth.
Choice C Reason: Abdominal breathing. This is not a sign of respiratory distress in newborns, but rather a normal patern of breathing for them. Abdominal breathing means that the newborn's abdomen rises and falls with each breath, which reflects the use of the diaphragm as the primary respiratory muscle.
Choice D Reason: Respiratory rate of 54 breaths/minute. This is not a sign of respiratory distress in newborns, but rather a normal range of respiratory rate for them. A normal respiratory rate for a newborn ranges from 40 to 60 breaths per minute.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: Respiratory rate of 16. This is an incorrect answer that indicates a normal finding that does not suggest magnesium sulfate toxicity. Respiratory rate is a measure of the number of breaths per minute, which reflects the respiratory function and oxygenation status. Respiratory rate of 16 is within the normal range for adults, which is 12 to 20 breaths per minute. Respiratory rate of 16 does not indicate magnesium sulfate toxicity, which can cause respiratory rate below 12 breaths per minute.
Choice B Reason: Complaints by the client of feeling flushed and warm. This is an incorrect answer that indicates a common side effect that does not indicate magnesium sulfate toxicity. Feeling flushed and warm are sensations that are caused by vasodilation (widening of blood vessels), which can occur as a result of magnesium sulfate administration. Feeling flushed and warm are not signs of magnesium sulfate toxicity, but rather expected and mild reactions that usually subside within a few hours.
Choice C Reason: Fetal heart rate of 120. This is an incorrect answer that indicates a normal finding that does not suggest magnesium sulfate toxicity. Fetal heart rate is a measure of the number of beats per minute of the fetal heart, which reflects the fetal well-being and oxygenation status. Fetal heart rate of 120 is within the normal range for fetuses, which is 110 to 160 beats per minute. Fetal heart rate of 120 does not indicate magnesium sulfate toxicity, which can cause fetal heart rate below 110 beats per minute or above 160 beats per minute.
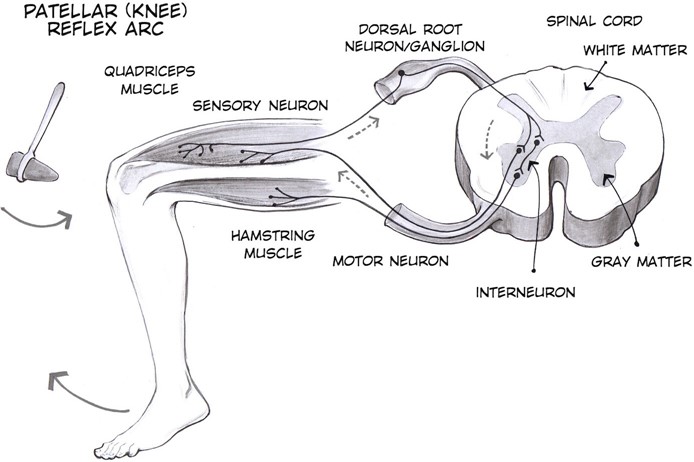
Choice D Reason: Patellar reflexes are absent. This is because absent patellar reflexes are a sign of magnesium sulfate toxicity, which is a condition where the level of magnesium in the blood is too high, which can cause adverse effects on the neuromuscular and cardiovascular systems. Magnesium sulfate is a medication that is used to prevent or treat preterm labor, which is labor that occurs before 37 weeks of gestation. Magnesium sulfate works by relaxing the uterine muscles and inhibiting uterine contractions. However, magnesium sulfate can also affect other muscles and nerves in the body, and cause symptoms such as muscle weakness, respiratory depression, hypotension, or cardiac arrest.
Correct Answer is C
Explanation
Choice A Reason: Late decelerations. This is an incorrect answer that refers to a different type of fetal heart rate patern that indicates uteroplacental insufficiency, which can reduce blood flow and oxygen delivery to the fetus. Late decelerations are characterized by gradual decreases in fetal heart rate that begin after the peak of uterine contractions and return to baseline after the end of contractions. Amnioinfusion is not effective for late decelerations, as it does not address the underlying cause of uteroplacental insufficiency, which may be due to maternal hypertension, diabetes, preeclampsia, or placental abruption.
Choice B Reason: Moderate decelerations. This is an incorrect answer that refers to a non-existent type of fetal heart rate patern, as there is no such term as moderate decelerations. The term moderate refers to the category of fetal heart rate variability, which is a measure of the fluctuations in fetal heart rate around the baseline. Moderate variability indicates normal fetal oxygenation and well-being, while absent or minimal variability indicates fetal hypoxia or distress.
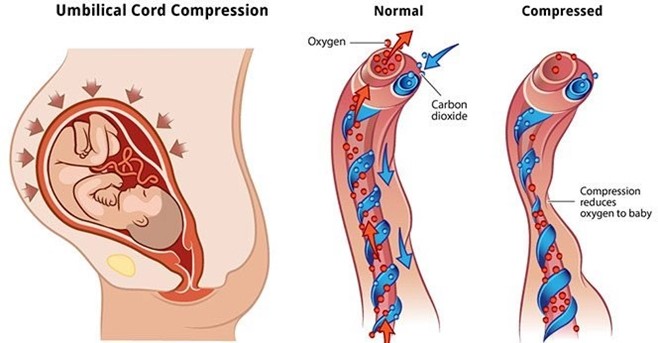
Choice C Reason: Variable decelerations. This is because variable decelerations are a type of fetal heart rate patern that indicates cord compression, which can reduce blood flow and oxygen delivery to the fetus. Variable decelerations are characterized by abrupt decreases in fetal heart rate that vary in onset, depth, and duration, and do not have a consistent relationship with uterine contractions. Amnioinfusion is a procedure that involves infusing saline or lactated Ringer's solution into the amniotic cavity through a transcervical catheter, which can relieve cord compression by increasing the volume of amniotic fluid and cushioning the cord. Amnioinfusion can improve fetal oxygenation and reduce variable decelerations.
Choice D Reason: Early decelerations. This is an incorrect answer that refers to a different type of fetal heart rate patern that indicates head compression, which can stimulate the vagus nerve and slow down the fetal heart rate. Early decelerations are characterized by gradual decreases in fetal heart rate that begin with the onset of uterine contractions and return to baseline with the end of contractions. Early decelerations are benign and do not require intervention, as they reflect normal fetal head descent and progress of labor. Amnioinfusion is not indicated for early decelerations, as it does not affect head compression or vagal stimulation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today