A client who is newly diagnosed with type 2 diabetes mellitus (DM) receives a prescription for metformin 500 mg PO twice daily. Which statement(s) should the nurse include in this client’s teaching plan? (Select all that apply.)
Take metformin with the morning and evening meal.
Use sliding scale insulin for frequent blood glucose elevations.
Recognize signs and symptoms of hypoglycemia.
Report persistent polyuria to the health care provider.
Take an additional dose for signs of hyperglycemia.
Correct Answer : A,C,D
Choice A reason: Taking metformin with the morning and evening meal is a correct statement for the nurse to include, as this can improve the absorption and effectiveness of metformin and reduce the risk of gastrointestinal side effects. Therefore, this is a correct choice.
Choice B reason: Using sliding scale insulin for frequent blood glucose elevations is not a correct statement for the nurse to include, as this is not recommended for clients with type 2 DM who are taking metformin. This can cause hypoglycemia and complicate the management of blood glucose levels. This is an incorrect choice.
Choice C reason: Recognizing signs and symptoms of hypoglycemia is a correct statement for the nurse to include, as this can help the client identify and treat low blood glucose levels, which can occur with metformin use or other factors such as exercise, fasting, or alcohol intake. Therefore, this is another correct choice.
Choice D reason: Reporting persistent polyuria to the health care provider is a correct statement for the nurse to include, as this can indicate poor glycemic control or a complication of DM such as diabetic ketoacidosis or nephropathy. Therefore, this is another correct choice.
Choice E reason: Taking an additional dose for signs of hyperglycemia is not a correct statement for the nurse to include, as this can cause overdose or toxicity of metformin, which can lead to lactic acidosis and renal failure. This is another incorrect choice.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
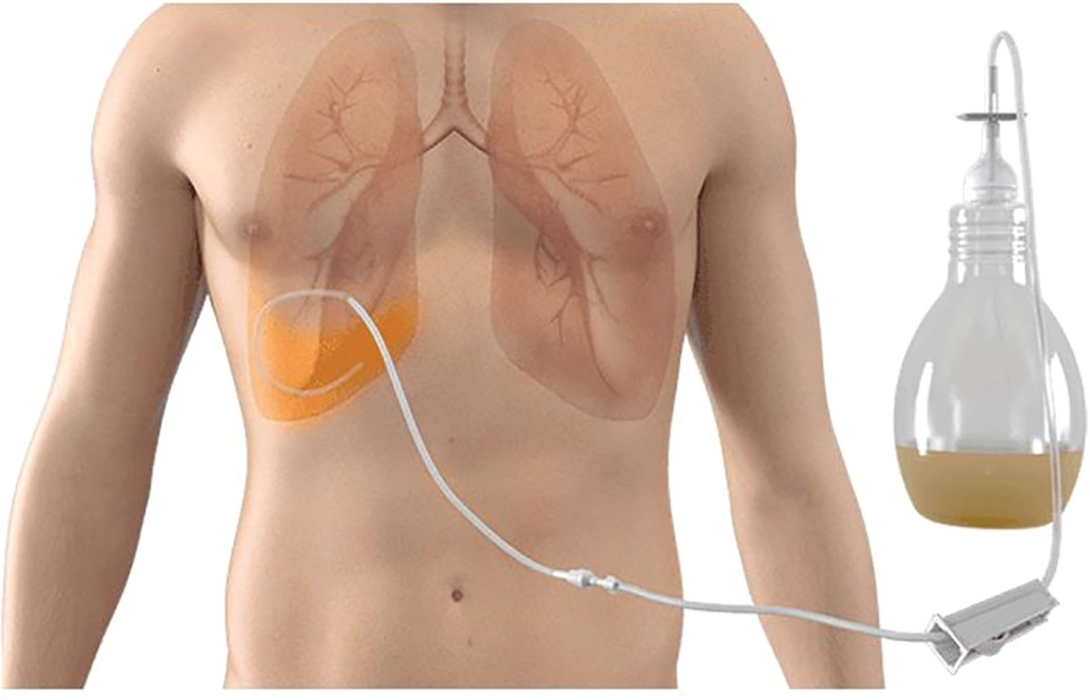
Choice A reason: Securing chest tube to the stretcher for transport is not the most important action for the nurse to take. Chest tube is a device that drains air or fluid from the pleural space or mediastinum after surgery or trauma. Securing chest tube to the stretcher can prevent accidental dislodgement or kinking of the tube during transport, but it is not as crucial as maintaining proper drainage.
Choice B reason: Administering PRN pain medication prior to transport is not the most important action for the nurse to take. Pain medication is a drug that relieves pain by blocking pain signals or reducing inflammation. Administering pain medication prior to transport can improve comfort and reduce anxiety for the client, but it is not as urgent as preventing complications.
Choice C reason: Marking the amount of chest drainage on the container is not the most important action for the nurse to take. Chest drainage is the fluid or air that collects in the chest tube container after being drained from the pleural space or mediastinum. Marking the amount of chest drainage on the container can help monitor fluid balance and detect excessive bleeding or leakage, but it is not as vital as ensuring proper drainage.
Choice D reason: This is the correct answer because keeping chest tube container below the site of insertion is the most important action for the nurse to take. Chest tube container is a device that collects air or fluid from the chest tube and maintains negative pressure in the pleural space or mediastinum. Keeping chest tube container below the site of insertion can prevent backflow of air or fluid into the chest cavity and maintain adequate drainage. If the chest tube container is raised above the site of insertion, it can cause tension pneumothorax, which is a life-threatening condition that occurs when air accumulates in the pleural space and compresses the lung and heart.
Correct Answer is ["B","C","D","E"]
Explanation
Choice A reason: This is incorrect because instructing the client and family to reconsider end of life choices is disrespectful and insensitive. The nurse should respect the client's autonomy and preferences and support their decisions.
Choice B reason: This is correct because teaching the client how to use guided imagery is a helpful intervention for coping with feelings related to death and dying. Guided imagery is a relaxation technique that involves visualizing positive images and scenarios that can reduce stress, anxiety, and pain.
Choice C reason: This is correct because recording the client's desire to live is an important intervention for coping with feelings related to death and dying. The nurse should acknowledge and validate the client's emotions and help them express their hopes and fears.
Choice D reason: This is correct because encouraging family to visit frequently is a beneficial intervention for coping with feelings related to death and dying. The nurse should facilitate family involvement and communication and help the client maintain meaningful relationships.
Choice E reason: This is correct because encouraging family to bring the client old photographs is a useful intervention for coping with feelings related to death and dying. The nurse should assist the client in reminiscing and reviewing their life story and achievements.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today