The nurse enters the room of an older adult client and observes the client positioned in a wheelchair as seen in the picture. The unlicensed assistive personnel (UAP) is preparing to push the client's wheelchair in the hallway. Which instruction should the nurse provide the UAP before the client is moved into the hallway?
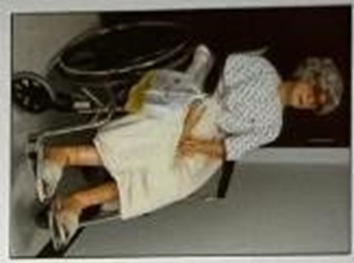
Use a belt restraint to secure the client in the chair.
Empty the client's urinary drainage bag.
Reposition the client's urinary drainage bag.
Elevate the client's feet higher on the foot rests.
The Correct Answer is C
A. Using a belt restraint is generally not recommended unless specifically ordered for safety reasons, as it may not be appropriate or necessary in all cases. Restraints should only be used when absolutely needed and when all other methods of ensuring safety have been considered.
B. Emptying the urinary drainage bag before moving the client is important to prevent overflows and ensure that the bag does not become a source of discomfort or potential infection. However, this step might not always be immediately necessary unless the bag is full or the client’s comfort and hygiene are at risk.
C. Repositioning the urinary drainage bag is crucial for ensuring that the bag remains below the level of the bladder and is not subject to kinks or obstructions. This helps prevent backflow and potential infections. Proper positioning also contributes to the client’s comfort and dignity, making this a priority before moving the client.
D. Elevating the client’s feet on the footrests is important for their comfort and to prevent swelling or pressure sores, especially if the client has limited mobility or circulatory issues. Proper positioning can prevent discomfort and promote better circulation, which is essential for maintaining the client’s well- being during transport.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. This can strain the back and increase the risk of injury. It's important to use proper body mechanics, such as bending the knees and keeping the back straight, when reaching for objects.
B. Bending at the waist can strain the back and increase the risk of injury. It's important to lift objects with the legs, not the back.
C. This can strain the back and hips. It's important to use proper body mechanics, such as using the legs and core muscles to push or pull heavy objects.
D. Standing erect with knees bent provides a strong base of support and helps to distribute weight evenly. Bending the knees allows for lifting with the legs, which is less stressful on the back and reduces the risk of injury. Pulling a draw sheet and moving a client in bed requires a combination of strength and proper body mechanics. Standing erect with knees bent helps to prevent strain on the back and muscles
Correct Answer is B
Explanation
A. While documenting the color and clarity of the urine is important for assessing the client's urinary output and potential issues, it is not the immediate next step in the catheter insertion process. This step typically comes after the catheter is fully inserted and secured.
B. Once urine flow is observed, the next step is to inflate the balloon of the indwelling catheter to secure it in place within the bladder. This ensures the catheter remains correctly positioned and does not move out of the bladder, which is crucial for effective drainage and preventing accidental dislodgement.
C. Asking the client to breathe deeply and exhale does not impact the catheterization process and is not related to the next immediate step after observing urine flow. This action might be helpful in other contexts, such as reducing anxiety or discomfort, but it does not address the technical steps required for catheter insertion.
D. If urine flow is observed in the catheter, it indicates that the catheter is already in the bladder. Inserting the catheter an additional inch is unnecessary and could potentially cause trauma or discomfort. Proper catheter placement is confirmed by the observation of urine flow, and additional insertion is not required.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today