The nurse is assessing the carotid arteries of a client with cardiovascular disease. What action should be performed next by the nurse?
Discuss that a light will be directed at the neck to observe for pulsations of the artery
instruct the client to take a deep breath and "hold" while the nurse briefly auscultates
Demonstrate that both arteries will be palpated simultaneously to compare amplitude
Show the client the diaphragm of the stethoscope that will be placed on the neck
The Correct Answer is C
A. Discuss that a light will be directed at the neck to observe for pulsations of the artery:
This choice is incorrect. Directing light at the neck is not a standard method for assessing carotid artery pulsations. The carotid artery is usually assessed by palpation to feel the pulse rather than visual observation.
B. Instruct the client to take a deep breath and "hold" while the nurse briefly auscultates:
This choice is incorrect. Auscultation is typically not used to assess carotid artery pulsations. Palpation (feeling the pulse) is the primary method used for this assessment.
C. Demonstrate that both arteries will be palpated simultaneously to compare amplitude:
This choice is correct. Palpating both carotid arteries simultaneously allows the nurse to compare the amplitude (strength) of the pulses. This comparison helps in assessing the symmetry of the pulses and ensures there are no significant differences between the two sides, which could indicate vascular abnormalities.
D. Show the client the diaphragm of the stethoscope that will be placed on the neck:
This choice is incorrect. The diaphragm of the stethoscope is not typically used for palpating pulses. Palpation involves using the fingertips to feel the pulse and assess its strength and regularity.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
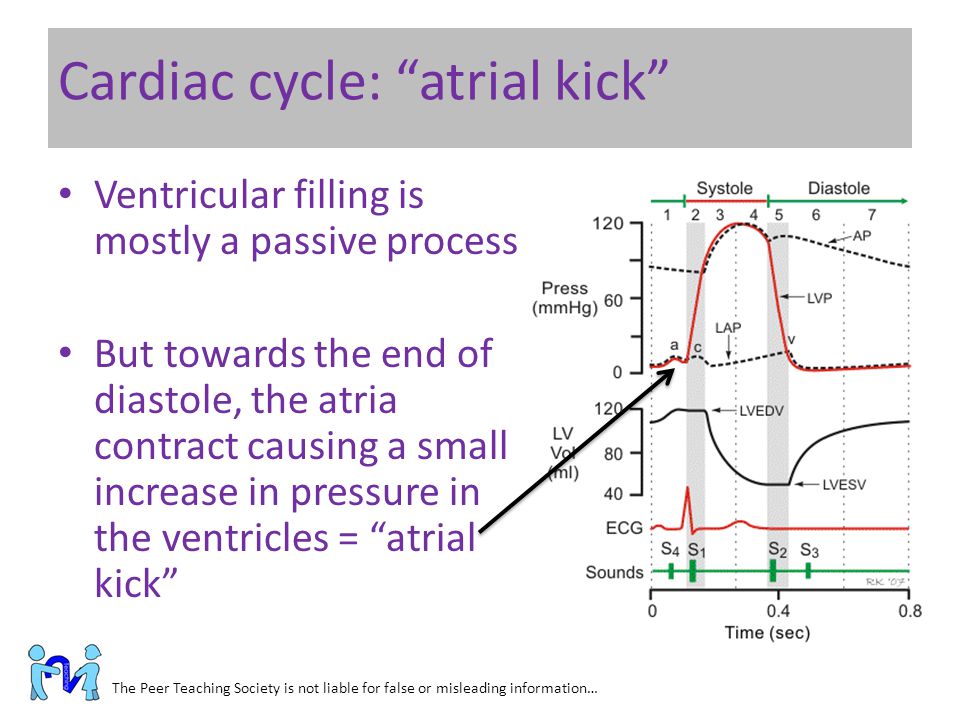
A. The atria contract toward the end of diastole and push the remaining blood into the ventricles.
This choice is correct. During atrial systole (atrial contraction), the atria contract, pushing the remaining blood into the ventricles. This additional filling of the ventricles optimizes cardiac output.
B. The atria contract during systole and attempt to push against closed valves.
This statement is incorrect. The atria do not contract during systole; they contract during diastole (atrial systole) to fill the ventricles.
C. Atrial kick is the pressure exerted against the atria as the ventricles contract during systole.
This statement is incorrect. Atrial kick refers to the atrial contraction, not the pressure exerted against the atria.
D. Contraction of the atria at the beginning of diastole can be felt as a palpitation.
This statement is not entirely accurate. A palpitation is a sensation of rapid or strong heartbeat, which might be felt during various cardiac events, not specifically during atrial contraction at the beginning of diastole.
Correct Answer is C
Explanation
A. Nystagmus in extreme superior gaze: Nystagmus is an involuntary eye movement and is not a normal finding, especially in extreme superior gaze. Nystagmus can be indicative of neurological issues and requires further evaluation.
B. Slight amount of lid lag when moving the eyes from a superior to an inferior position: Lid lag refers to a delay in the downward movement of the upper eyelid during eye movement. This can be a sign of hyperthyroidism and is not a normal finding.
C. Parallel movement of both eyes: This is the correct answer. During the diagnostic positions test, the nurse should observe parallel movement of both eyes in all directions, indicating normal extraocular muscle function and coordination.
D. Convergence of the eyes: Convergence refers to the inward movement of both eyes when focusing on a close object. While convergence is a normal phenomenon, it is not specifically assessed during the diagnostic positions test, which primarily evaluates the range of motion and coordination of the extraocular muscles.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today