The nurse is preparing to assess the visual acuity of an adult client. Which of the following assessment should the nurse use for visual acuity?
Perform the confrontation test.
Ask the patient to read the print on a handheld Jaeger card.
Determine the patient's ability to read newsprint at a distance of 12 to 14 inches.
Use the Snellen chart positioned 20 feet away from the patient.
The Correct Answer is D
A. Perform the confrontation test:
The confrontation test is a basic visual field screening test. It assesses the peripheral vision by having the patient cover one eye and the examiner covers the opposite eye. The patient and the examiner then bring their fingers into the visual field from the periphery, and the patient indicates when they see the fingers.
B. Ask the patient to read the print on a handheld Jaeger card:
Jaeger cards are used for near vision testing. The patient reads progressively smaller print to assess their near vision acuity.
C. Determine the patient's ability to read newsprint at a distance of 12 to 14 inches:
This method assesses near vision. It is often used informally in clinical settings, where the patient is asked to read a newspaper or similar print at a comfortable reading distance.
D. Use the Snellen chart positioned 20 feet away from the patient:
The Snellen chart is a standardized chart used for visual acuity testing. It is placed 20 feet away from the patient, and the patient is asked to read the letters or symbols on the chart with one eye covered at a time.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
. Presence of breath sounds: While assessing the anterior chest, the nurse should listen for breath sounds over various areas of the lungs. However, this is related to auscultation, not inspection.
B. Diaphragmatic excursion: Diaphragmatic excursion involves assessing the movement of the diaphragm during breathing. This is typically done by percussing the level where dullness changes to resonance during inhalation and exhalation. It is more related to percussion, not inspection.
C. Symmetric chest expansion: Symmetric chest expansion refers to the equal expansion of both sides of the chest during inhalation. The nurse can observe and palpate the chest to assess if it expands symmetrically on both sides. This is a crucial aspect of the inspection of the anterior chest.
D. Shape and configuration of the chest wall: The shape and configuration of the chest wall, including abnormalities or deformities, should be assessed during inspection. This includes observing for any asymmetry, deformities, masses, or scars on the anterior chest.
Correct Answer is B
Explanation
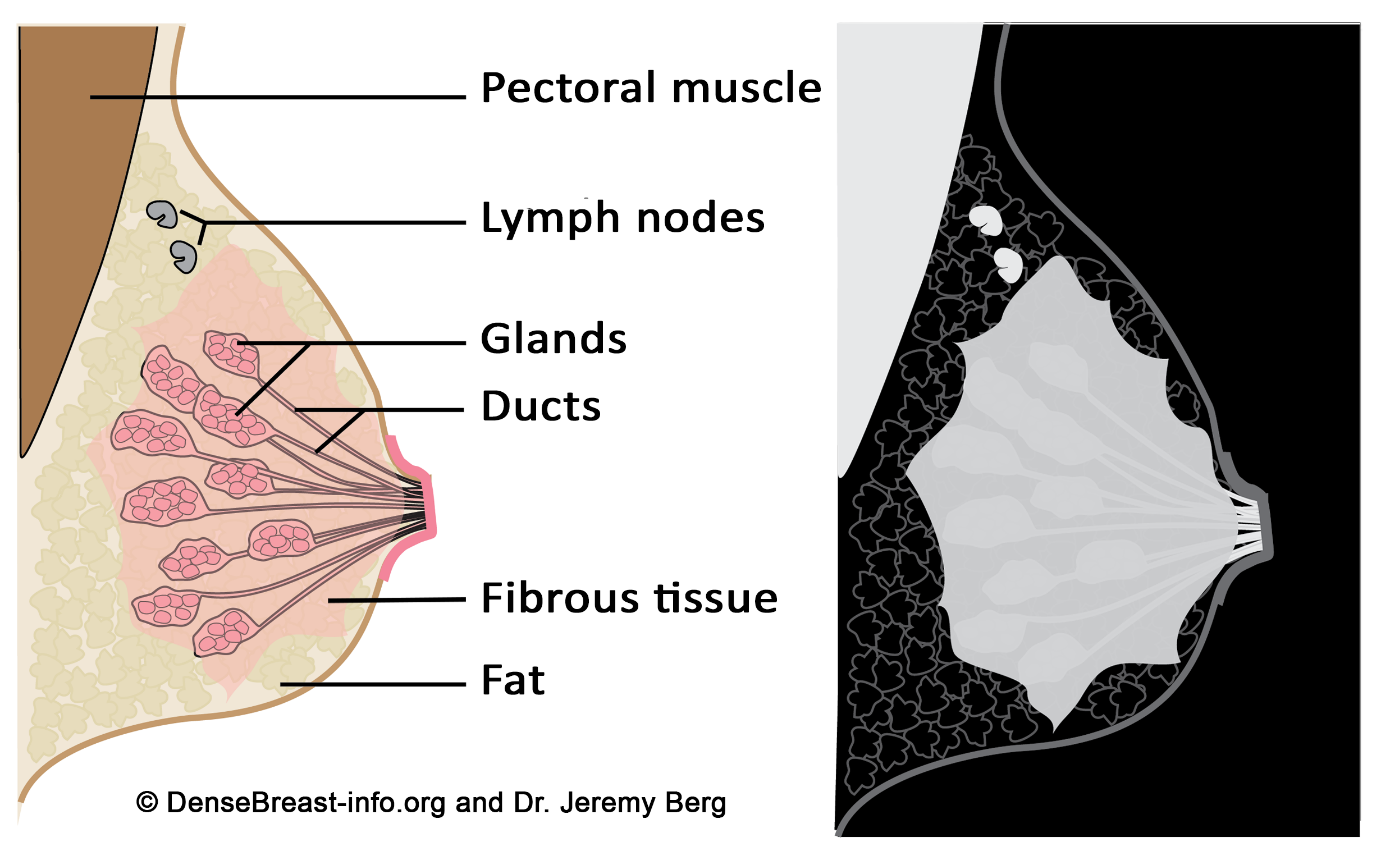
A. Glandular tissue, which supports the breast by attaching to the chest wall: Glandular tissue is indeed a part of the breast structure, but it is not responsible for supporting the breast by attaching to the chest wall. It's the Cooper's ligaments, which are fibrous connective tissue, that provide structural support.
B. Fibrous, glandular, and adipose tissues: This statement is correct. The breast is composed of glandular tissue (responsible for milk production), fibrous tissue (including Cooper's ligaments for support), and adipose tissue (fat).
C. Primarily muscle with very little fibrous tissue: The breast contains very little muscle tissue. The main supportive structure is fibrous tissue, not muscle.
D. Primarily milk ducts, known as lactiferous ducts: Milk ducts are part of the glandular tissue and are responsible for carrying milk. However, the breast is not primarily made up of milk ducts; it consists of a combination of glandular, fibrous, and adipose tissues.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today