The nurse is caring for a child with suspected diabetes insipidus. Which clinical manifestation would be observable?
Oliguria
Glycosuria
Nausea and vomiting
Polydipsia
The Correct Answer is D
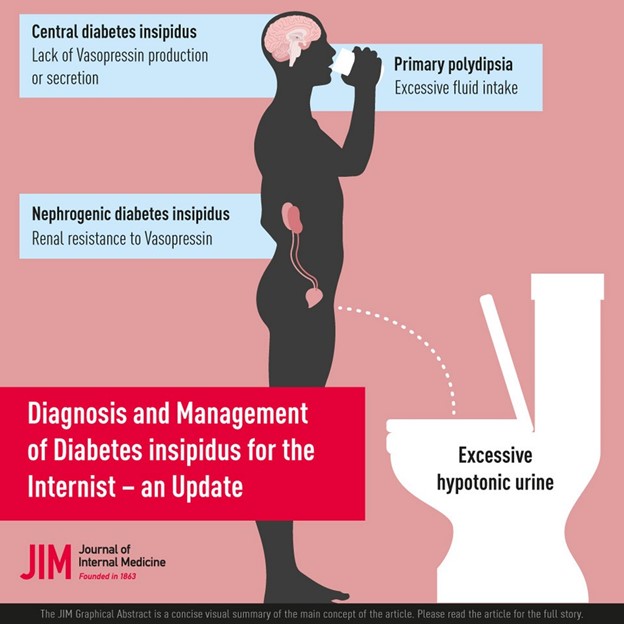
Diabetes insipidus is a disorder of the posterior pituitary gland that causes a deficiency of antidiuretic hormone (ADH). This leads to excessive urination (polyuria) and excessive thirst (polydipsia) as the body tries to balance the fluid loss. These symptoms may be so severe that the child does little other than drink and urinate.
Choice A is wrong because oliguria means decreased urine production and is not associated with diabetes insipidus.
Choice B is wrong because glycosuria means glucose in the urine and is associated with diabetes mellitus, not diabetes insipidus.
Choice C is wrong because nausea and vomiting are associated with inappropriate ADH secretion (SIADH), which causes fluid retention and hyponatremia, not diabetes insipidus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Diabetes insipidus is a disorder of the posterior pituitary gland that causes a deficiency of antidiuretic hormone (ADH). This leads to excessive urination (polyuria) and excessive thirst (polydipsia) as the body tries to balance the fluid loss. These symptoms may be so severe that the child does little other than drink and urinate.
Choice A is wrong because oliguria means decreased urine production and is not associated with diabetes insipidus.
Choice B is wrong because glycosuria means glucose in the urine and is associated with diabetes mellitus, not diabetes insipidus.
Choice C is wrong because nausea and vomiting are associated with inappropriate ADH secretion (SIADH), which causes fluid retention and hyponatremia, not diabetes insipidus.
Correct Answer is D
Explanation
choice D. Monitor blood glucose levels frequently and observe closely for signs of hypoglycemia. This is because a macrosomic infant (a newborn who’s much larger than average) is at risk of developing low blood sugar levels after birth, especially if the mother has diabetes. Hypoglycemia can cause neurological damage in the newborn, so it is important to detect and treat it promptly.
Choice A is wrong because leaving the infant in the room with the mother without monitoring the blood glucose levels may miss signs of hypoglycemia and delay treatment.
Choice B is wrong because taking the infant immediately to the nursery may separate the infant from the mother and interfere with breastfeeding, which can help prevent hypoglycemia.
Choice C is wrong because performing a gestational age assessment to determine whether the infant is large for gestational age is not urgent and does not address the risk of hypoglycemia.
Normal ranges for blood glucose levels in term infants are 2.6 mmol/L or higher at any time. A blood glucose level of 2.5 mmol/L or less is considered hypoglycemic.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today