The nurse is testing a client's visual accommodation. Which of the following should the nurse recognize as an assessment finding from visual accommodation?
The pupils constrict when the examiner's index finger slowly moves toward the client's nose.
The client involuntary blinks in the presence of bright light directed over the pupils during the eye exam.
The client's peripheral vision becomes sharper when the examiner shines a light over the pupils.
The pupils dilate when the examiner's index finger slowly moves toward the client's nose.
The Correct Answer is A
A. The pupils constrict when the examiner's index finger slowly moves toward the client's nose.
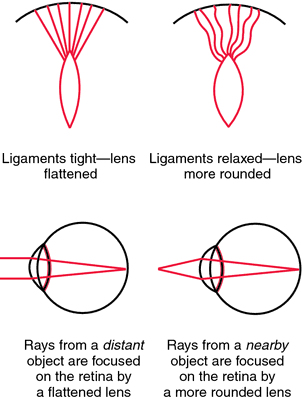
This statement is correct. Visual accommodation is the process by which the eye's lens changes shape to focus on objects at varying distances. When an object moves closer to the eyes, the pupils constrict to adjust and focus on the near object, preventing double vision.
B. The client involuntarily blinks in the presence of bright light directed over the pupils during the eye exam.
This statement describes the pupillary light reflex, not visual accommodation. The pupillary light reflex is the response of the pupils to light exposure.
C. The client's peripheral vision becomes sharper when the examiner shines a light over the pupils.
This statement is not accurate. Peripheral vision sharpness is not related to visual accommodation. Visual accommodation mainly involves adjusting focus for objects at varying distances.
D. The pupils dilate when the examiner's index finger slowly moves toward the client's nose.
This statement is incorrect. Pupils should constrict, not dilate, when focusing on a near object (as in visual accommodation). Dilation occurs in low-light conditions or in response to sympathetic stimulation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is {"dropdown-group-1":"C"}
Explanation
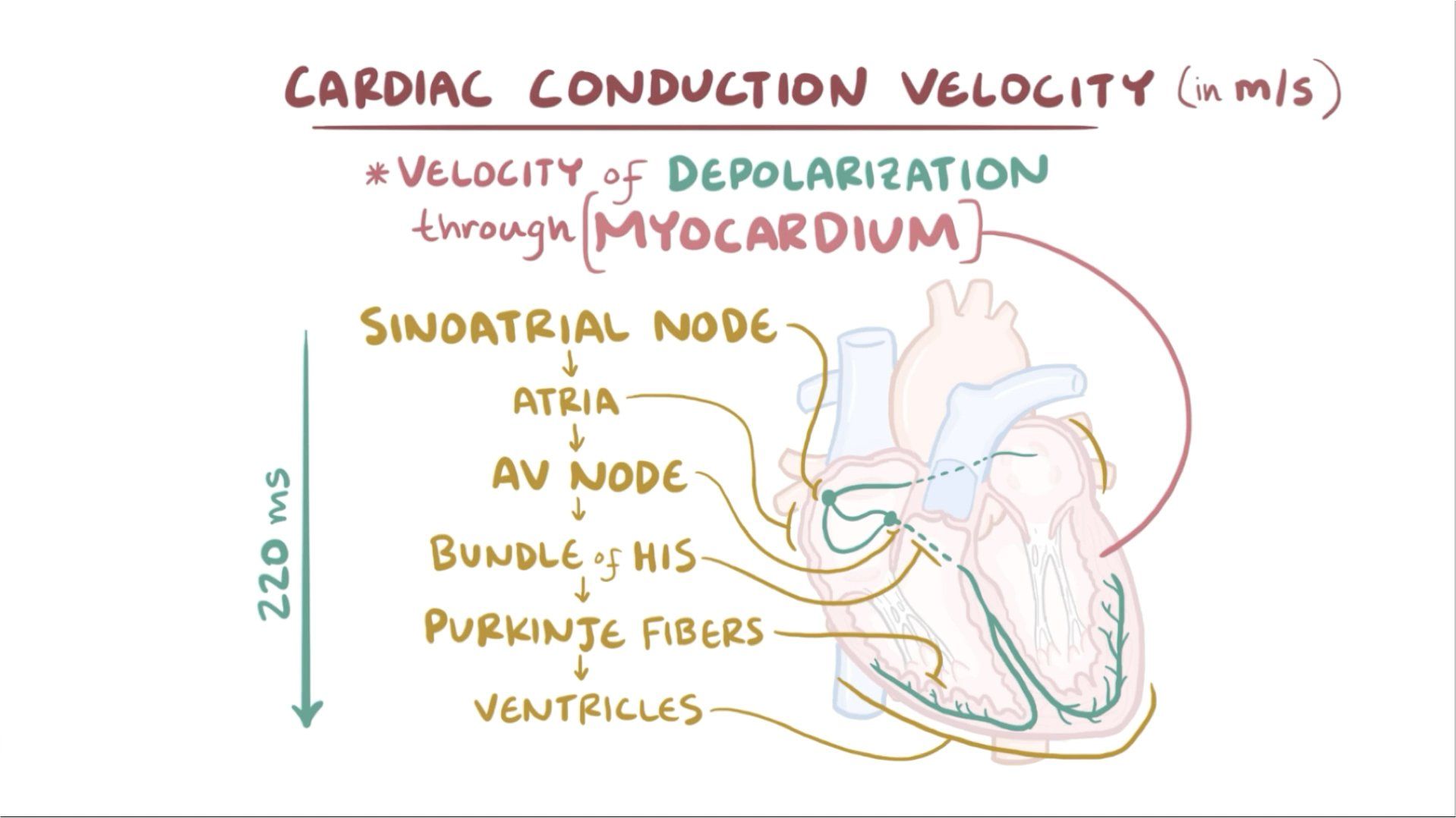
The pacemaker of the heart is known as the sinoatrial (SA) node. The SA node is a specialized group of cells located in the right atrium of the heart. It generates electrical impulses that initiate each heartbeat and set the rhythm for the entire heart.
Correct Answer is C
Explanation
A. VI
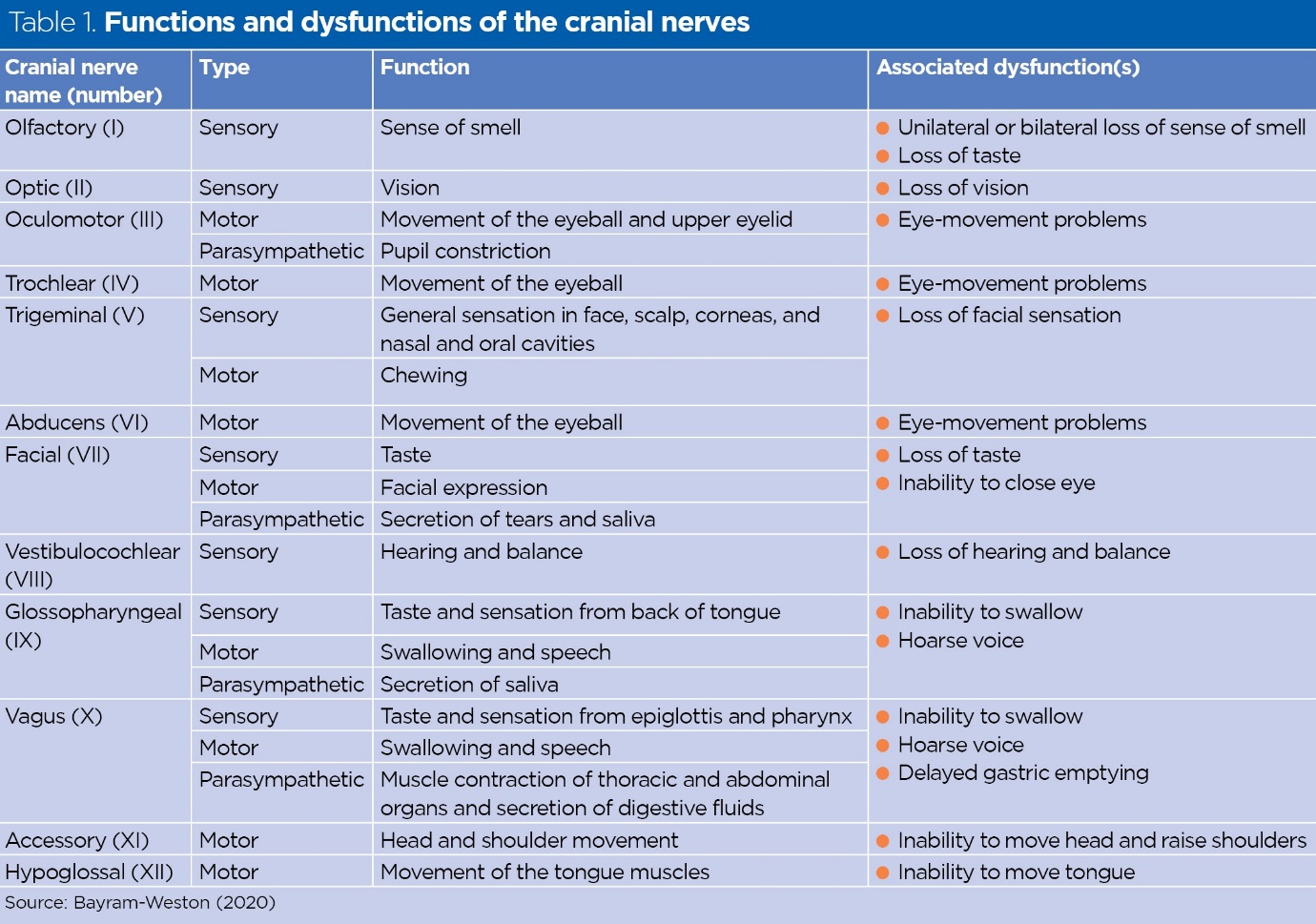
Cranial Nerve VI is the Abducent Nerve, which controls the movement of the lateral rectus muscle, allowing the eye to move laterally (abduct). Dysfunction of this nerve can cause difficulty in moving the eye outward.
B. V
Cranial Nerve V is the Trigeminal Nerve. It has both sensory and motor functions. Sensory functions include providing sensation to the face, sinuses, and teeth. Motor functions include controlling the muscles used for chewing (mastication).
C. II
Cranial Nerve II is the Optic Nerve. It is purely a sensory nerve responsible for vision. The optic nerve carries visual information from the retina of the eye to the brain.
D. III
Cranial Nerve III is the Oculomotor Nerve. It is primarily a motor nerve but also has some autonomic functions. It controls most of the eye movements (except lateral movement controlled by VI) and regulates the size of the pupil and the shape of the lens in the eye for focusing.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today