The nurse observes that the tissue over the sacrum is dark, hard, and adherent to the wound edge. What is the stage for this pressure injury?
Stage IV
Stage II
Stage III
Unstageable
The Correct Answer is D
D. Unstageable pressure injuries are covered by slough (yellow, tan, gray, green, or brown) and/or eschar (tan, brown, or black) in the wound bed, making it difficult to determine the depth of tissue damage. If the wound over the sacrum is covered with dark, hard tissue that makes it impossible to visualize the depth of the wound, it could be considered unstageable
A. The description of tissue over the sacrum being dark, hard, and adherent to the wound edge suggests extensive tissue damage and possibly involvement of deeper structures like muscle or bone.
B. Stage II pressure injuries involve partial-thickness loss of skin with exposed dermis. These wounds are shallow and typically present as abrasions, blisters, or shallow ulcers.
C. Stage III pressure injuries involve full-thickness skin loss with visible adipose (fat) tissue in the ulcer. These wounds may also have undermining or tunneling.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","E"]
Explanation
A. This is located on the lateral side of the thigh. It is a commonly used site for infants, toddlers, and young children, as well as adults who require large-volume injections.
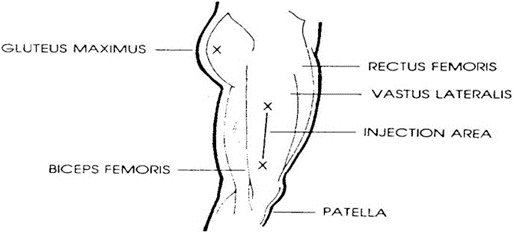
B. This site is located on the hip or gluteal region. It is considered one of the safest and least painful sites for intramuscular injections in adults. It is also used when the volume of medication is larger or when the dorsogluteal site is contraindicated.
E. This site is located on the upper arm, specifically the lateral aspect. It is commonly used for vaccines and medications that require smaller volumes in adults and older children.
C. There is no specific muscle called the "rectus lateralis." It seems to be a combination of the rectus femoris (a muscle in the quadriceps group of the thigh) and the vastus lateralis. However, neither "rectus lateralis" nor "rectus femoris" is commonly used as a distinct injection site in clinical practice.
D. This site is located on the buttocks. Historically, it was a commonly used site for intramuscular injections, but it has fallen out of favor due to the potential risk of injury to the sciatic nerve and superior gluteal artery.
Correct Answer is A
Explanation
A. This is the most direct and appropriate question to assess for dysuria. Dysuria is characterized by pain, discomfort, or burning sensation during urination. Asking this question helps the nurse to directly assess if the client is experiencing these symptoms.
B. This question is more relevant for assessing urinary frequency rather than dysuria. It is important for assessing other urinary symptoms but does not specifically address the characteristic pain or discomfort associated with dysuria.
C. This question is pertinent for assessing urinary retention or incomplete emptying of the bladder, which are different concerns from dysuria. It evaluates the client's perception of bladder emptying rather than pain or discomfort during urination.
D. This question is more relevant for assessing urinary hesitancy or urgency, which are related to bladder function but are not specific to dysuria. It addresses issues with urine flow dynamics rather than pain or discomfort during urination.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today