The nurse on a urology unit is caring for a client diagnosed with calcium oxalate renal calculi.
When planning this client's health education, what nutritional guidelines should the nurse provide?
Increase purine-rich food intake.
Follow a low-calcium diet.
Increase intake of potassium-rich foods.
Restrict foods with protein.
The Correct Answer is D

Protein intake can increase the excretion of calcium and oxalate in the urine, which can promote the formation of calcium oxalate stones. The client should limit animal protein sources, such as meat, poultry, fish, eggs, and dairy products.
Choice A is wrong because purine-rich foods, such as organ meats, shellfish, and beer, can increase the production of uric acid, which can cause uric acid stones.
Choice B is wrong because a low-calcium diet can increase the absorption of oxalate in the intestine, which can increase the risk of calcium oxalate stones.
The client should consume a moderate amount of calcium from dietary sources, such as milk, cheese, yogurt, and green leafy vegetables.
Choice C is wrong because potassium-rich foods, such as bananas, oranges, potatoes, and tomatoes, can help prevent calcium oxalate stones by increasing the urinary pH and citrate levels.
The client should consume adequate amounts of potassium from dietary sources.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Increased urine output is a sign of adequate hydration, as it means the kidneys are filtering waste and fluids from the body through the urine. The urine should be pale straw or lemonade colored, which indicates good hydration.
Choice B is wrong because decreased urine output is a sign of dehydration, as it means the kidneys are not working well and waste products are accumulating in the blood.
The urine may be dark and strong smelling, which indicates poor hydration.
Choice C is wrong because dry mucous membranes are a sign of dehydration, as they indicate a lack of fluid in the body tissues.
Choice D is wrong because hypertension is not a direct indicator of hydration status, although dehydration can cause low BP due to reduced blood volume.
Correct Answer is A
Explanation
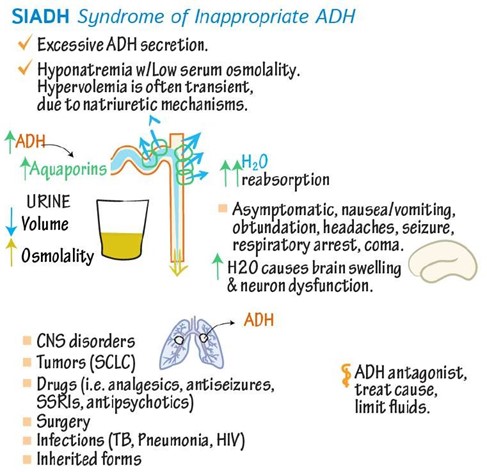
SIADH is a condition in which your body makes too much antidiuretic hormone (ADH), which controls how your body releases and conserves water.
SIADH makes it harder for your kidneys to release water and causes the levels of electrolytes, like sodium, to fall due to water retention.
This leads to hyponatremia, which is when you have low levels of sodium in your blood.
Choice B is wrong because hypernatremia is when you have high levels of sodium in your blood.
This can occur due to dehydration, excessive salt intake, or kidney problems.
Choice C is wrong because hyperkalemia is when you have high levels of potassium in your blood.
This can occur due to kidney failure, acidosis, or certain medications.
Choice D is wrong because hypokalemia is when you have low levels of potassium in your blood.
This can occur due to vomiting, diarrhea, diuretics, or alkalosis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today