Which is the hormone that stimulates the release of aldosterone from the adrenal cortex.
Renin.
Angiotensin I.
Angiotensin II.
Antidiuretic hormone (ADH).
The Correct Answer is C
Angiotensin II is a hormone that stimulates the adrenal cortex to release aldosterone. Aldosterone is a hormone that helps regulate blood pressure by increasing the reabsorption of sodium and water and the excretion of potassium by the kidneys.
Choice A is wrong because renin is not a hormone but an enzyme that catalyzes the conversion of angiotensinogen to angiotensin I1.
Choice B is wrong because angiotensin I is an inactive precursor of angiotensin II that is converted by angiotensin-converting enzyme (ACE) in the lungs.
Choice D is wrong because antidiuretic hormone (ADH) is a hormone that regulates water balance by increasing the reabsorption of water by the kidneys, but it does not affect aldosterone secretion.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
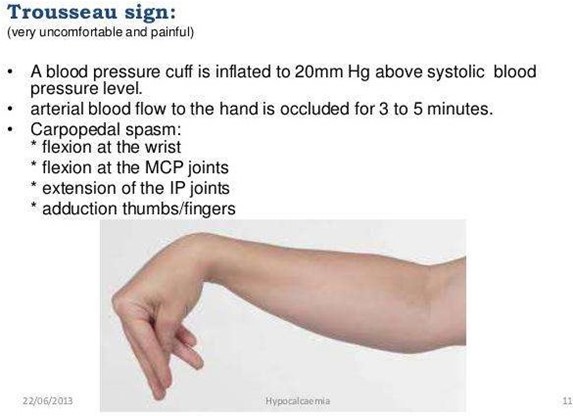
Trousseau’s sign is a test for hypocalcemia that involves inflating a blood pressure cuff on the arm and observing for carpal spasm. A positive sign indicates low calcium levels in the blood, which can cause neuromuscular irritability.
Choice B is wrong because hyperactive deep tendon reflexes are a sign of hypomagnesemia, which is a low level of magnesium in the blood.
Choice C is wrong because hyperactive bowel sounds are a sign of hyperkalemia, which is a high level of potassium in the blood.
Choice D is wrong because muscle twitching can be caused by many factors, such as anxiety, caffeine, or electrolyte imbalance, and is not specific to hypocalcemia.
Correct Answer is ["A","C","D"]
Explanation
Furosemide is a loop diuretic that causes the kidneys to excrete more water and salt, which can lead to dehydration and electrolyte imbalance.
Electrolyte imbalance can cause muscle cramps, numbness and tingling, weakness and fatigue, and other symptoms.
Therefore, the client should monitor for these signs and report them to the doctor if they occur.
Choice B is wrong because dry mouth is not a sign of electrolyte imbalance, but rather a sign of dehydration.
Dehydration can also cause thirst, decreased urination, drowsiness, and confusion.
Choice E is wrong because tachycardia is not a sign of electrolyte imbalance, but rather a sign of hypovolemia (low blood volume) or hypotension (low blood pressure).
Furosemide can lower blood pressure by reducing fluid volume in the body.
Therefore, the client should also monitor their blood pressure and pulse regularly while taking furosemide.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today