The public health nurse is assigned to the population of clients in an inner city community. The nurse identifies which of the following as a priority intervention.
Develop a survey on teen pregnancies
Hold a focus group to discuss immunizations
Interview the elderly at the senior center
Perform a windshield survey
The Correct Answer is D
Choice A reason: Developing a survey on teen pregnancies is not a priority intervention for a public health nurse who is assigned to a new community. This is a specific topic that may not be relevant or important for the whole population. A survey also requires time and resources to design, distribute, and analyze.
Choice B reason: Holding a focus group to discuss immunizations is not a priority intervention for a public health nurse who is assigned to a new community. This is a specific topic that may not be representative of the community's health needs and concerns. A focus group also requires recruitment, facilitation, and interpretation of the participants' views.
Choice C reason: Interviewing the elderly at the senior center is not a priority intervention for a public health nurse who is assigned to a new community. This is a specific group that may not reflect the diversity and characteristics of the whole population. An interview also requires consent, rapport, and recording of the responses.
Choice D reason: Performing a windshield survey is a priority intervention for a public health nurse who is assigned to a new community. This is a general method that allows the nurse to observe and assess various aspects of the environment that affect the health and well-being of the population. A windshield survey also requires minimal resources and can be done quickly and easily. A windshield survey is a method of assessing the health needs and resources of a community by driving or walking around and observing various aspects of the environment, such as housing, transportation, services, and safety. This is a priority intervention for a public health nurse who wants to get a comprehensive overview of the community and identify its strengths and weaknesses.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
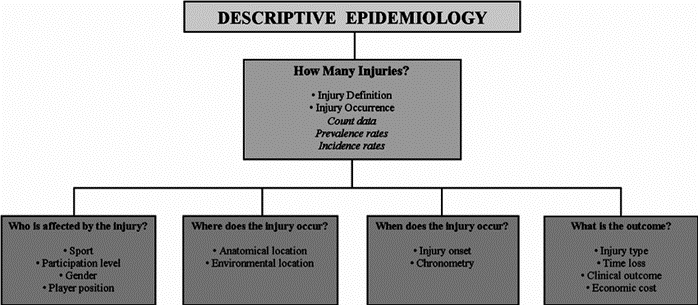
Choice A: Reviewing communicable disease statistics. This is incorrect because this is an example of descriptive epidemiology, not analytic epidemiology. Descriptive epidemiology describes the distribution and patterns of health events in populations, such as the frequency, location, and time of occurrence.
Choice B: Tracking locations where family violence is increasing. This is incorrect because this is also an example of descriptive epidemiology, not analytic epidemiology. Descriptive epidemiology tracks the trends and variations of health problems in different groups or areas.
Choice C: Describing population characteristics for healthy older citizens. This is incorrect because this is another example of descriptive epidemiology, not analytic epidemiology. Descriptive epidemiology provides information about the demographic and social factors that influence health outcomes.
Choice D: Identifying factors contributing to childhood obesity. This is correct because this is an example of analytic epidemiology. Analytic epidemiology investigates the causes and associations of health events in populations, such as the risk factors, exposures, or interventions that affect health outcomes. Analytic epidemiology often uses comparison groups to test hypotheses and draw conclusions.
Correct Answer is D
Explanation
Choice A: Administer corticosteroids. This is incorrect because corticosteroids are used to reduce inflammation and suppress the immune system, but they do not directly affect venous return, stiffness, or muscle strength and endurance.
Choice B: Turn and reposition every 2 hours. This is incorrect because turning and repositioning are important to prevent pressure ulcers and promote circulation, but they are not sufficient to maintain muscle strength and endurance. The client also needs active or passive exercises to prevent muscle atrophy and contractures.
Choice C: Administer interferon. This is incorrect because interferon is a type of immunomodulator that can reduce the frequency and severity of relapses in multiple sclerosis, but it does not directly affect venous return, stiffness, or muscle strength and endurance.
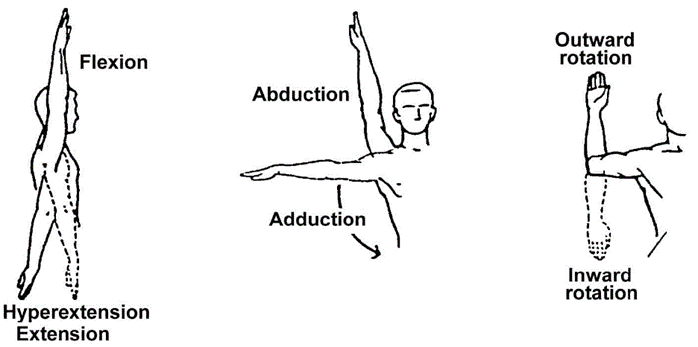
Choice D: Encourage range-of-motion exercises. This is correct because range-of-motion exercises can help increase venous return, prevent stiffness, and maintain muscle strength and endurance in clients with multiple sclerosis. Range-of-motion exercises can be performed actively by the client or passively by the nurse or a caregiver. They should be done at least twice a day to prevent complications such as contractures, spasticity, and pain.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today