What eye function is the nurse preparing to assess when the client is asked to stand 20 feet from a specific chart that is mounted on the examination room wall?
Peripheral vision.
External eye structures.
Distant vision.
Near vision.
The Correct Answer is C
Choice A reason:
Peripheral vision is the ability to see objects and movement outside of the direct line of vision. This type of vision is assessed using different methods, such as confrontation visual field testing, where the examiner moves objects into the patient's side vision from different angles. Standing 20 feet away from a chart would not be the appropriate method to assess peripheral vision.
Choice B reason:
The assessment of external eye structures involves examining the physical appearance and condition of the eyelids, sclera, conjunctiva, and surrounding areas. This is typically done at a close range and does not require the patient to stand at a distance from a chart. The nurse would inspect these structures directly, often with the aid of a penlight for better visibility.
Choice C reason:
Distant vision is the ability to see objects far away, and it is what the nurse is preparing to assess when the client is asked to stand 20 feet from a chart. This distance is standard for the Snellen eye chart, which is used to measure visual acuity. The chart has rows of letters that decrease in size, and the patient is asked to read the smallest line of letters they can see clearly. The Snellen chart is the most common method used by eye doctors to measure visual acuity.
Choice D reason:
Near vision is the ability to see objects that are close to the eyes clearly. It is assessed using different charts, such as the Jaeger eye chart, which contains blocks of text in various type sizes. The patient is asked to read the text at a close range, typically around 14 inches, not 20 feet. Therefore, standing 20 feet away from a chart would not be the method to assess near vision.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason:
The conjunctiva can sometimes appear yellow in individuals with jaundice; however, it is not the most reliable area to inspect for jaundice. The conjunctiva may be affected by other factors such as environmental irritants or infections, which can alter its appearance.
Choice B Reason:
The sclera of the eye is the most reliable area to inspect for jaundice. The yellowing of the sclera, also known as scleral icterus, is a key indicator of jaundice. The sclera's white background provides a clear contrast, making any yellow discoloration more noticeable. This is particularly true in darker-skinned individuals, where skin changes may be less apparent.
Choice C Reason:
The back of the neck is not a reliable area to inspect for jaundice. Skin pigmentation and lighting can affect the visibility of yellowing, making it an unreliable indicator. Additionally, the back of the neck may have other skin changes unrelated to jaundice that could confuse the assessment.
Choice D Reason:
The palms of the hands are not the most reliable area to inspect for jaundice. While the palms may show yellowing, they are subject to various external factors such as manual labor or exposure to substances that can affect their color. Moreover, the palms' skin may be thicker and less transparent, making subtle changes in color more difficult to detect.
Correct Answer is A
Explanation
Choice A Reason:
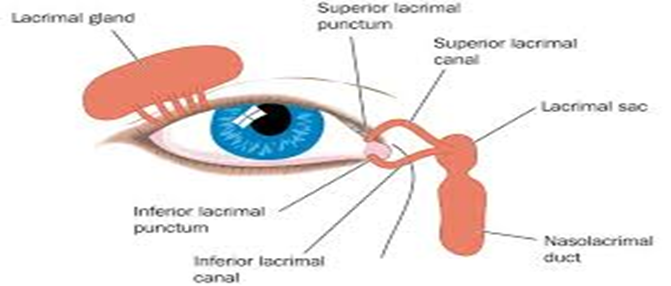
The nasolacrimal sac is part of the tear drainage system. When a patient presents with excessive tearing, known as epiphora, it is important to assess for any obstruction in the lacrimal apparatus. The nasolacrimal sac can become blocked due to various reasons such as infection, inflammation, or structural abnormalities. Assessing this area can help determine if there is a blockage causing the tears to accumulate and overflow.
Choice B Reason:
Inspecting the palpebral conjunctiva is typically done if there is a complaint of eye pain or a sensation of a foreign body in the eye. While it is part of a comprehensive eye examination, it is not the first assessment to be performed for excessive tearing unless there are additional symptoms that suggest a problem with the conjunctiva.
Choice C Reason:
Testing the pupillary reaction to light is an assessment of the pupillary response and the function of the oculomotor nerve. This test is crucial when neurological issues are suspected or if there is a change in vision. However, it is not the primary assessment for excessive tearing without other associated symptoms.
Choice D Reason:
The eye positions test, which assesses eye muscle strength and cranial nerve function, is not necessary unless there are signs of problems with muscle strength, such as drooping. This test would not typically be the next step in assessing a patient with excessive tearing unless there are other indications of muscle or nerve impairment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today