What would be considered early signs/symptoms of pressure injury (Stage 1)?
Intact skin with nonblanchable redness, painful,warm, soft localized area over a bony prominence
Shallow, open, shiny, dry injury, pink-red wound bed without sloughing or bruising
Full-thickness tissue loss, slough and black eschar in wound bed with undermining and tunneling
Full-thickness tissue loss, subcutaneous fat visible, possible undermining and tunneling
The Correct Answer is A
A. Intact skin with nonblanchable redness, painful, warm, soft localized area over a bony prominence
Stage 1 pressure injuries are characterized by intact skin with nonblanchable redness over a localized area, typically over a bony prominence like the sacrum, heel, or elbow. The skin may feel painful, warm, and soft to the touch. Nonblanchable redness means that when pressure is applied to the area, the redness does not fade or blanch (turn white). This stage indicates that tissue damage has occurred, but the skin is still intact.
B. Shallow, open, shiny, dry injury, pink-red wound bed without sloughing or bruising: This description is more indicative of a Stage 2 pressure injury, which involves partial-thickness skin loss with an intact or ruptured blister. The wound bed is usually pink or red, and there is no sloughing or bruising.
C. Full-thickness tissue loss, slough and black eschar in wound bed with undermining and tunneling: This description corresponds to a Stage 3 or Stage 4 pressure injury. Stage 3 involves full-thickness tissue loss with visible subcutaneous fat but no bone, tendon, or muscle exposed. Stage 4 involves extensive tissue loss with exposure of bone, tendon, or muscle. Both stages may include slough (yellow or white tissue) and black eschar (hard, necrotic tissue), along with undermining (tissue destruction under intact skin edges) and tunneling (narrow passageways extending from the wound).
D. Full-thickness tissue loss, subcutaneous fat visible, possible undermining and tunneling: This description also corresponds to a Stage 3 pressure injury, as it involves full-thickness tissue loss with visible subcutaneous fat. The mention of possible undermining and tunneling further suggests a Stage 3 pressure injury.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
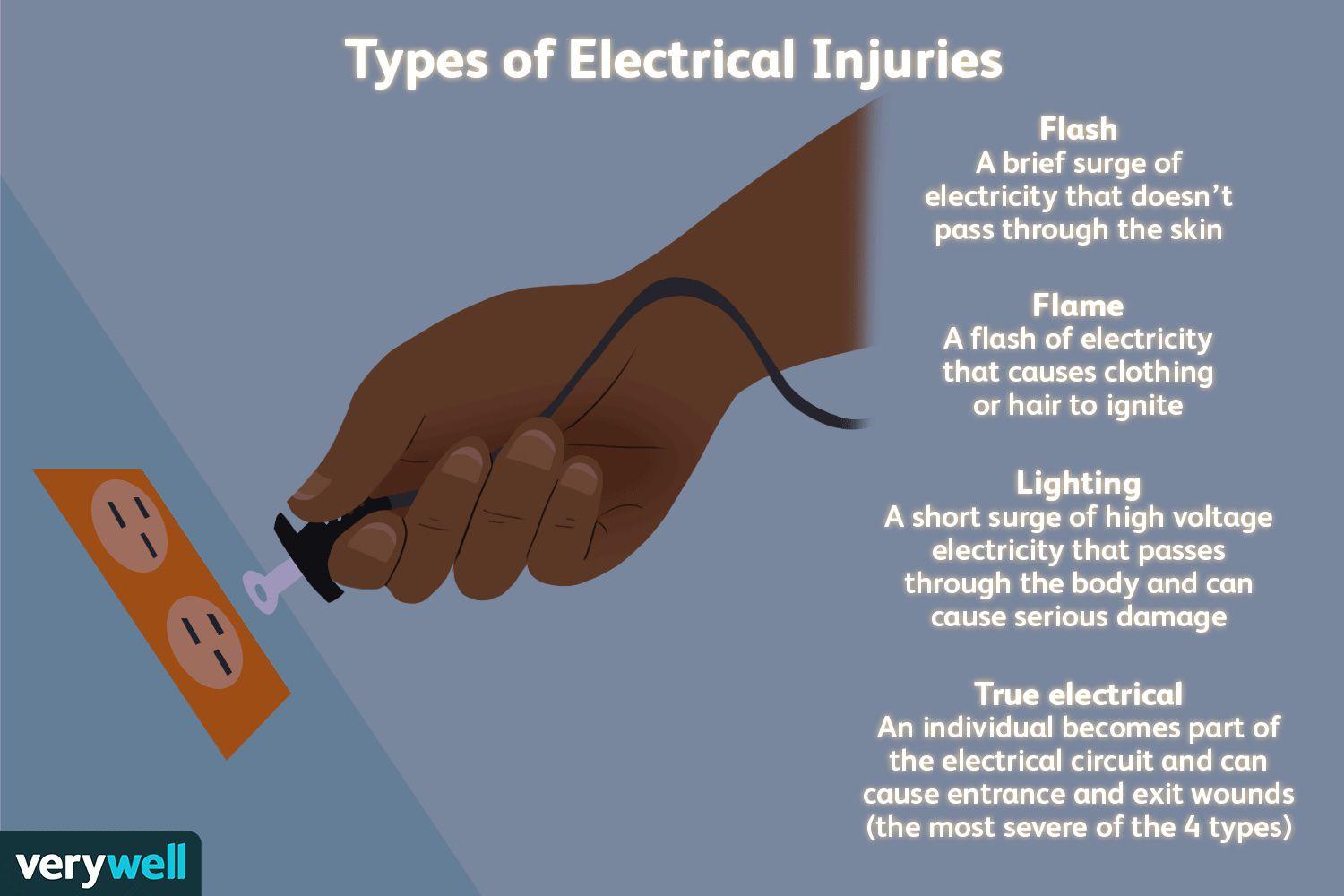
A. Electrical burns can have small amounts of skin damage, but more extensive damage beneath the skin.
This response is the best choice because it educates the client about the potential for deeper tissue damage associated with electrical burns. It acknowledges that while the burn on the skin may appear small, the damage underneath could be more extensive, affecting muscles, nerves, and blood vessels.
B. Electrical burns commonly cause reddened/purplish skin without blistering.
This statement is not the best response because it focuses solely on the appearance of the skin without addressing the potential for deeper tissue damage. While it is true that electrical burns can present with reddened or purplish skin without blistering, this response does not provide comprehensive information about the nature and severity of electrical burns.
C. Electrical burns typically are minor.
This response is incorrect because it downplays the seriousness of electrical burns. While some electrical burns may indeed be minor, others can cause significant tissue damage and complications. It's important for the nurse to educate the client about the range of severity that electrical burns can present.
D. Electrical burns usually cause much more skin damage than what can be seen on your skin.
This statement is partially accurate but does not provide as much information as choice A. While it acknowledges that electrical burns can cause more damage than what is visible on the skin's surface, it doesn't emphasize the potential for deeper tissue damage as effectively as choice A does.
Correct Answer is B
Explanation
A. Metabolic acidosis:
Metabolic acidosis is characterized by a low pH (<7.35) and a low bicarbonate level (<22 mEq/L) due to an excess of acids in the body or a loss of bicarbonate. However, in the given ABG values, the pH is low (7.22), but the bicarbonate level is elevated (28 mEq/L), which does not align with metabolic acidosis. Therefore, metabolic acidosis is not the correct interpretation in this case.
B. Respiratory acidosis:
Respiratory acidosis occurs when there is inadequate removal of carbon dioxide (CO2) by the lungs, leading to an accumulation of CO2 in the blood and a decrease in pH. In the ABG values provided, the pH is low (7.22), and the PaCO2 is elevated (68 mm Hg), indicating respiratory acidosis as the primary disturbance. This interpretation is supported by the elevated PaCO2 and the low pH, making it the correct choice based on the given data.
C. Respiratory alkalosis:
Respiratory alkalosis results from hyperventilation, leading to excessive elimination of CO2 and a decrease in PaCO2 levels. However, in the ABG values presented, the PaCO2 is elevated (68 mm Hg), which contradicts the expected decrease seen in respiratory alkalosis. Therefore, respiratory alkalosis is not the correct interpretation of the ABG values in this case.
D. Metabolic alkalosis:
Metabolic alkalosis is characterized by a high pH (>7.45) and a high bicarbonate level (>26 mEq/L) due to excessive loss of acids or an increase in bicarbonate levels. However, in the ABG values provided, the pH is low (7.22), and the bicarbonate level is elevated (28 mEq/L), which is not consistent with metabolic alkalosis. Therefore, metabolic alkalosis is not the correct interpretation based on the given data.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today