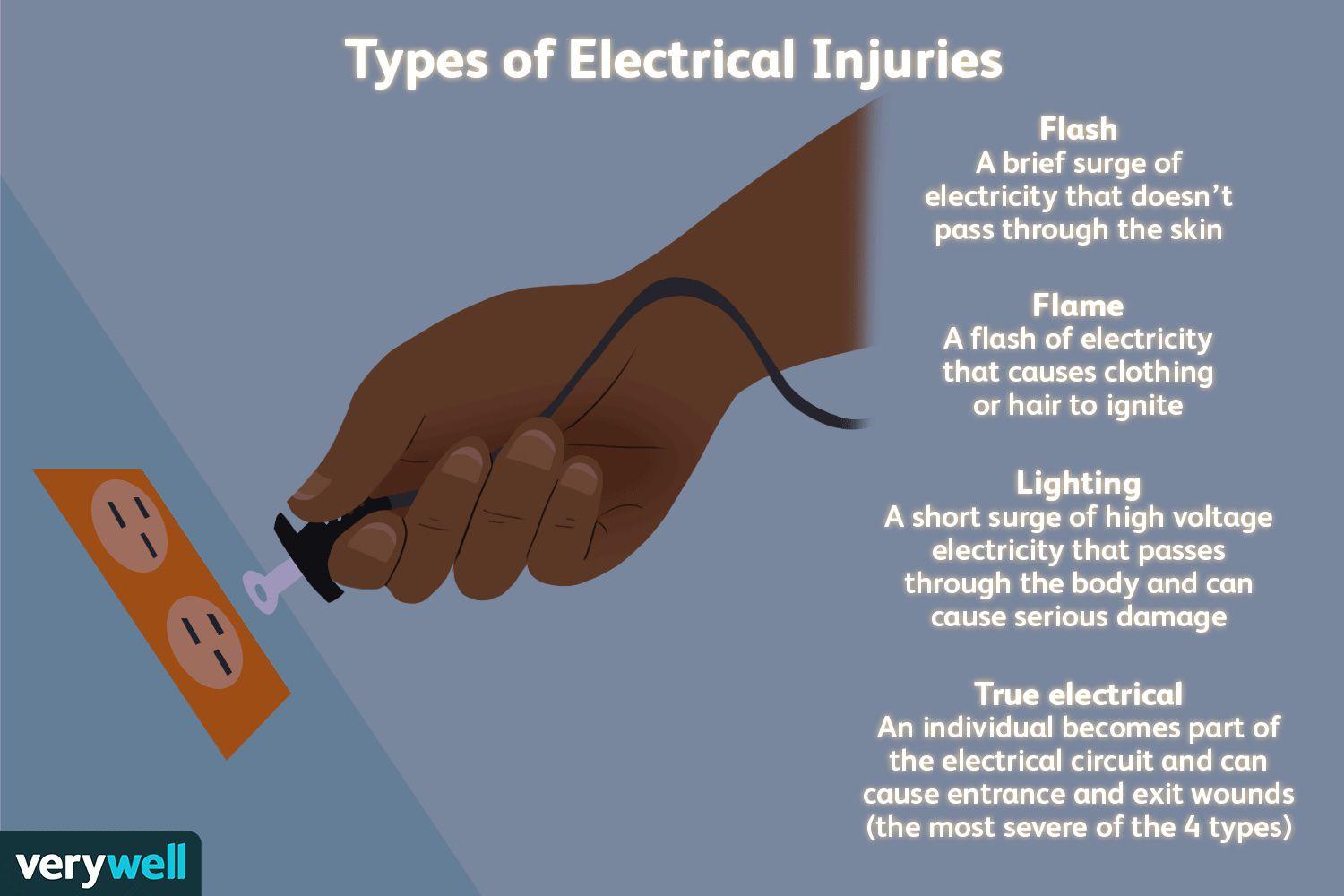
A nurse is caring for a client with an electrical burn. The client states that since the wound on the skin is small, the burn must not be too bad. Which of the following is the best response by the nurse?
Electrical burns can have small amounts of skin damage, but more extensive damage beneath the skin.
Electrical burns commonly cause reddened/purplish skin without blistering.
Electrical burns typically are minor.
Electrical burns usually cause much more skin damage than what can be seen on your skin.
The Correct Answer is A
A. Electrical burns can have small amounts of skin damage, but more extensive damage beneath the skin.
This response is the best choice because it educates the client about the potential for deeper tissue damage associated with electrical burns. It acknowledges that while the burn on the skin may appear small, the damage underneath could be more extensive, affecting muscles, nerves, and blood vessels.
B. Electrical burns commonly cause reddened/purplish skin without blistering.
This statement is not the best response because it focuses solely on the appearance of the skin without addressing the potential for deeper tissue damage. While it is true that electrical burns can present with reddened or purplish skin without blistering, this response does not provide comprehensive information about the nature and severity of electrical burns.
C. Electrical burns typically are minor.
This response is incorrect because it downplays the seriousness of electrical burns. While some electrical burns may indeed be minor, others can cause significant tissue damage and complications. It's important for the nurse to educate the client about the range of severity that electrical burns can present.
D. Electrical burns usually cause much more skin damage than what can be seen on your skin.
This statement is partially accurate but does not provide as much information as choice A. While it acknowledges that electrical burns can cause more damage than what is visible on the skin's surface, it doesn't emphasize the potential for deeper tissue damage as effectively as choice A does.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Change the dressing when it is saturated:
This intervention is the most appropriate for managing a deep wound with a wet to-damp dressing. Wet to-damp dressings are designed to maintain a moist environment conducive to wound healing. Changing the dressing when it becomes saturated with wound exudate helps prevent excessive moisture accumulation, which can lead to skin maceration and potential infection. It ensures that the wound bed remains in an optimal healing environment and reduces the risk of complications.
B. Assess the wound bed once a day:
Assessing the wound bed is an essential part of wound care, as it allows the nurse to monitor healing progress, assess for signs of infection, and evaluate the effectiveness of the chosen dressing. However, the frequency of wound bed assessment may vary depending on the specific patient's needs and the type of dressing being used. While daily assessment is generally recommended, it does not directly dictate the timing of dressing changes for wet to-damp dressings, which are primarily changed based on saturation levels.
C. Contact the provider when the dressing leaks:
Contacting the provider when the dressing leaks or when there are concerns or complications is an important step in patient care. Leaking dressings can indicate issues with the dressing application, excessive wound exudate, or potential complications such as infection. It's crucial to inform the provider promptly so that appropriate interventions can be implemented, but this instruction is more reactive and does not specifically address the timing of dressing changes.
D. Change the dressing every 6 hours:
Changing the dressing every 6 hours is not typically recommended for wet to-damp dressings unless specifically indicated based on the patient's condition and the amount of wound exudate. Frequent dressing changes can disrupt the healing process, cause unnecessary trauma to the wound bed, and increase the risk of infection. Dressing change frequency should be based on the assessment of wound exudate and the dressing's ability to maintain a moist environment.
Correct Answer is C
Explanation
A. “All preoperative patients get this medication.” This statement is too broad and not entirely accurate. While many preoperative patients do receive famotidine (Pepcid), it’s not a standard for all. Medications are prescribed based on individual patient needs and medical history.
B. “The physician prescribed this medication for you.” While this is technically true, it doesn’t provide the patient with an understanding of why the medication is necessary. As a nurse, part of your role is to educate patients about their medications.
C. “It helps prevent ulcers from the stress of the surgery.” This is the correct answer. Famotidine (Pepcid) is given to decrease the amount of acid produced in the stomach, which can help prevent stress ulcers that can occur due to the physical stress of surgery.
D. “Since you don’t have ulcers, I will have to ask.” This statement suggests uncertainty and a lack of knowledge about the medication’s purpose. It’s important for healthcare professionals to understand the medications they administer and be able to explain them to patients.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today