Which assessment finding of an older adult living in an assisted-living facility indicates the highest risk for suicide?
Older adult declines company, is preoccupied with lethal weapons.
Liver failure is due to alcohol abuse, older adult is popular at meals.
Refuses to allow a large, extended family to help him.
The older adult had an overdose of acetaminophen 20 years ago; is in a sewing group.
None of the above.
The Correct Answer is A
Choice A reason: Older adult declines company, is preoccupied with lethal weapons is the highest risk factor for suicide, as it indicates social isolation, hopelessness, and suicidal intent. The older adult may be suffering from depression, anxiety, or other mental health issues that impair their quality of life and increase their likelihood of harming themselves.
Choice B reason: Liver failure is due to alcohol abuse, older adult is popular at meals is not the highest risk factor for suicide, as it does not indicate suicidal ideation or behavior. The older adult may have a chronic medical condition that affects their liver function, but they may also have a supportive social network and coping skills that reduce their risk of suicide.
Choice C reason: Refuses to allow a large, extended family to help him is not the highest risk factor for suicide, as it does not indicate suicidal ideation or behavior. The older adult may have a preference for independence and autonomy, or they may have a strained relationship with their family. However, they may also have other sources of support and meaning in their life that lower their risk of suicide.
Choice D reason: The older adult had an overdose of acetaminophen 20 years ago; is in a sewing group is not the highest risk factor for suicide, as it does not indicate current suicidal ideation or behavior. The older adult may have a history of a suicide attempt, but they may also have recovered from their past crisis and found a positive outlet for their emotions and interests in the sewing group.
Choice E reason: None of the above is not the correct answer, as there is one choice that indicates the highest risk for suicide.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","D"]
Explanation
Choice A: Protect the skin from trauma. This is a correct answer. Purpura is the discoloration of the skin or mucous membranes due to hemorrhage from small blood vessels¹. It can be caused by various factors, such as blood clotting disorders, medications, infections, or weak blood vessels². Older adults are more prone to develop purpura because their skin becomes thinner and more fragile with age³. Therefore, protecting the skin from trauma, such as knocking against hard surfaces, can help prevent or reduce purpura.
Choice B: Remind the health care personnel to be gentle when handling this client’s skin. This is also a correct answer. Health care personnel should be aware of the risk of purpura in older adults and handle their skin with care. They should avoid applying excessive pressure, friction, or shear forces to the skin, as these can cause damage to the blood vessels and result in purpura. They should also use soft and smooth materials, such as cotton or silk, when dressing or cleaning the skin.
Choice C: Wear a long-sleeved shirt. This is not a correct answer. Wearing a long-sleeved shirt may provide some protection to the skin, but it is not enough to prevent purpura. Moreover, wearing tight or rough clothing can actually worsen the condition by causing irritation or injury to the skin. Therefore, this is not a good advice for the client.
Choice D: Tape a nonadherent dressing over the site of a skin tear. This is another correct answer. A skin tear is a type of wound that occurs when the skin is separated from the underlying tissue, usually due to trauma. Skin tears are common in older adults and can lead to purpura if the blood vessels are damaged. Taping a nonadherent dressing over the site of a skin tear can help protect the wound from infection, promote healing, and prevent further bleeding.
Correct Answer is ["A","C","D"]
Explanation
Choice A: Increase in physical activity
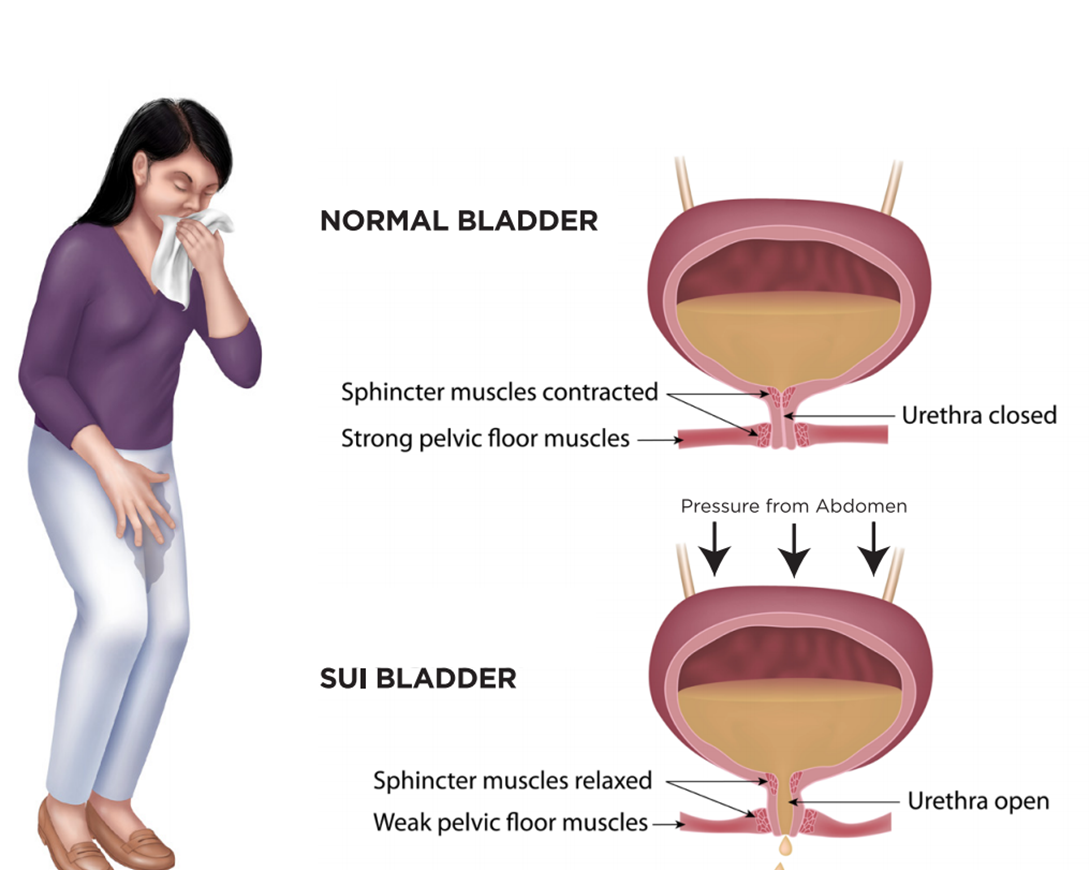
Physical activity can strengthen the muscles that help control urination. Exercises such as Kegels can specifically target these muscles, leading to improvements in urinary incontinence.
Choice B: Blood sugar control
While blood sugar control is important for overall health and can prevent complications from diabetes, it is not directly associated with improvements in urinary incontinence.
Choice C: Smoking cessation
Smoking can lead to coughing which puts pressure on the bladder and can exacerbate symptoms of urinary incontinence. Therefore, smoking cessation can lead to improvements.
Choice D: Weight reduction
Excess weight can put pressure on the bladder and surrounding muscles. Losing weight can reduce this pressure and improve symptoms of urinary incontinence.
There is no Choice E in this case. Each of these interventions can contribute to overall health and may indirectly affect urinary incontinence, but Choices A, C, and D are the most directly related to improvements in this condition.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today