While performing a routine assessment, a nurse notices fraying on the electrical cord of a client’s continuous passive motion (CPM) device.
Which of the following actions should the nurse take first?
Report the defect to the equipment maintenance staff.
Remove the device from the room.
Initiate a requisition for a replacement CPM device.
Ensure the device inspection sticker is current.
The Correct Answer is B
The correct answer is b. Remove the device from the room.
Choice A rationale:
- Reporting the defect to the equipment maintenance staff is essential, but it's not the immediate priority. The primary concern is to eliminate the safety hazard posed by the frayed cord to prevent potential harm to the client and others.
- Delaying the removal of the device could lead to electrical shock, fire, or other serious consequences.
- Therefore, removing the device from the room takes precedence over reporting the defect.
Choice B rationale:
- Removing the device from the room is the most appropriate first action because it:
- Eliminates the immediate safety hazard.
- Prevents potential harm to the client and others.
- Protects the device from further damage.
- Ensures the safety of the environment.
- Demonstrates the nurse's prioritization of patient safety.
Choice C rationale:
- Initiating a requisition for a replacement CPM device is necessary to ensure the client's continued treatment.
- However, it's not the first action because it doesn't address the immediate safety concern.
- The nurse should first remove the faulty device and then initiate the process for obtaining a replacement.
Choice D rationale:
- Ensuring the device inspection sticker is current is a vital part of equipment maintenance.
- However, it's not relevant to the immediate safety issue of the frayed cord.
- The presence of a current inspection sticker doesn't guarantee the device's safety or functionality at that moment.
- The nurse must prioritize removing the hazard and then follow up with appropriate documentation and reporting.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
This is a sign of preeclampsia, a serious complication of pregnancy that can cause high blood pressure, proteinuria, and seizures.
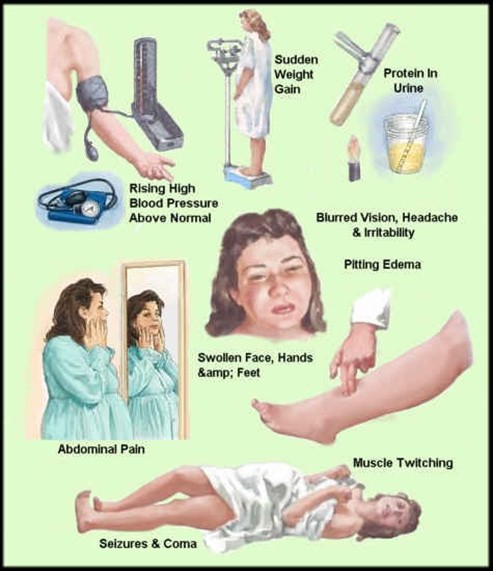
Preeclampsia can affect the placenta, the kidneys, the liver, and the brain of the mother and the fetus. It requires immediate medical attention and may lead to early delivery.
Choice A, bleeding gums, is wrong because it is a common occurrence during pregnancy due to hormonal changes that increase blood flow to the gums. It is not a cause for concern unless it is excessive or accompanied by other symptoms.
Choice B, urinary frequency, is wrong because it is also a normal finding during pregnancy due to the growing uterus putting pressure on the bladder. It is not a sign of infection or kidney problems unless it is associated with pain, burning, or blood in the urine.
Choice D, faintness upon rising, is wrong because it is usually caused by orthostatic hypotension, a drop in blood pressure when changing positions.
This can happen during pregnancy due to the dilation of blood vessels and the increased blood volume. It can be prevented by rising slowly, drinking enough fluids, and avoiding prolonged standing.
Correct Answer is D
Explanation
The correct answer is choiced. A client who is taking warfarin and has an INR of 1.8.
Choice A rationale:
An induration after a Mantoux test indicates a positive reaction, but it does not necessarily require immediate follow-up unless the induration is significant and the client has risk factors for tuberculosis.
Choice B rationale:
Sodium phosphate is commonly used as a bowel preparation for colonoscopy. This does not typically require follow-up unless the client experiences adverse effects such as dehydration or electrolyte imbalance.
Choice C rationale:
A potassium level of 3.6 mEq/L is within the normal range (3.5-5.0 mEq/L). Therefore, this finding does not require follow-up.
Choice D rationale:
An INR of 1.8 for a client taking warfarin is below the therapeutic range for most indications (typically 2.0-3.0). This requires follow-up to adjust the warfarin dosage to achieve the desired anticoagulation effect.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today