
Ati Nurs 140 Proctored Exam Maternal Newborn
Ati Nurs 140 Proctored Exam Maternal Newborn
Total Questions : 40
Showing 10 questions Sign up for moreA nurse is caring for a client who is a primigravida, at term, and having contractions but is stating that she is "not really sure if she is in labor or not." Which of the following should the nurse recognize as a sign of true labor?
Explanation
Choice A rationale
As labor begins, the cervix starts to soften, shorten and thin (efface). This process is often expressed in percentages¹. This is a sign of true labor².
Choice B rationale
The station of the presenting part refers to the position of the baby's head in relation to the mother's pelvis. While it can indicate progress in labor, it is not a definitive sign of true labor.
Choice C rationale
Rupture of the membranes, or water breaking, can occur before or during labor. However, it is not a reliable sign of true labor as it can also occur in preterm labor or even without contractions.
Choice D rationale
The pattern of contractions can be a sign of labor. True labor contractions are regular, increase in intensity, and do not ease up with change in activity or position². However, contractions alone are not a definitive sign of true labor as they can also occur in false labor (Braxton Hicks contractions).

A nurse is caring for a client who is in labor and has an epidural anesthesia block. The client's blood pressure is 80/40 mm Hg and the fetal heart rate is 140/min. Which of the following is the priority nursing action?
Explanation
Choice A rationale
This is incorrect because monitoring vital signs every 5 min is not the priority action. The client's blood pressure is low, indicating hypotension, which is a common complication of epidural anesthesia. Hypotension can compromise the placental blood flow and fetal oxygenation, so the nurse should act quickly to correct it.
Choice B rationale
This is incorrect because elevating the client's legs is not the priority action. Elevating the legs can increase venous return and cardiac output, but it can also worsen the hypotension by pooling blood in the lower extremities. The nurse should lower the head of the bed and place the client in a lateral position to improve blood pressure and fetal perfusion.
Choice C rationale
This is incorrect because notifying the provider is not the priority action. The nurse should first implement interventions to correct the hypotension, such as placing the client in a lateral position, administering oxygen, and increasing IV fluids. The nurse should notify the provider after stabilizing the client's condition or if the interventions are ineffective.
Choice D rationale
This is correct because placing the client in a lateral position is the priority action. This helps to relieve the pressure of the gravid uterus on the inferior vena cava and improve venous return, cardiac output, and blood pressure. It also enhances placental blood flow and fetal oxygenation, which are vital for a successful labor and delivery.
A nurse is caring for a client who is in the first stage of labor, undergoing external fetal monitoring, and receiving IV fluid. The nurse observes variable decelerations in the fetal heart rate on the monitor strip. Which of the following is a correct interpretation of this finding?
Explanation
Choice A rationale
This is incorrect because variable decelerations are not related to fetal head compression. Fetal head compression causes early decelerations, which are symmetrical and mirror the shape of the uterine contraction.
Choice B rationale
This is correct because variable decelerations are due to umbilical cord compression. Umbilical cord compression reduces the blood flow and oxygen delivery to the fetus, resulting in abrupt and irregular decreases in the fetal heart rate that vary in onset, depth, and duration.
Choice C rationale
This is incorrect because variable decelerations are not caused by uteroplacental insufficiency. Uteroplacental insufficiency causes late decelerations, which are symmetrical and begin after the peak of the uterine contraction.
Choice D rationale
This is incorrect because variable decelerations are not a result of the administration of narcotic analgesics. Narcotic analgesics can cause a decrease in the baseline fetal heart rate and variability, but not variable decelerations.
A nurse in a prenatal clinic is caring for a client. Using Leopold maneuvers, the nurse palpates a round, firm, movable part in the fundus of the uterus and a long, smooth surface on the client's right side. In which abdominal quadrant should the nurse expect to auscultate fetal heart tones?
Explanation
Choice A rationale
This is incorrect because the right upper quadrant is not the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the same side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
Choice B rationale
This is incorrect because the left upper quadrant is not the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the opposite side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
Choice C rationale
This is incorrect because the left lower quadrant is not the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the opposite side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
Choice D rationale
This is correct because the right lower quadrant is the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the same side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
A nurse is caring for a client who is postoperative following a tracheostomy, and has copious and tenacious secretions. Which of the following is an acceptable method for the nurse to use to thin this client's secretions?
Explanation
A. Provide humidified oxygen.
Humidified oxygen adds moisture to the air, which can help to thin secretions in the airway. Thinning the secretions makes them easier to clear, particularly for patients with copious and tenacious secretions, such as those following a tracheostomy.
B. Perform chest physiotherapy prior to suctioning.
Chest physiotherapy techniques, such as percussion and vibration, can help to mobilize secretions in the lungs and airways. While this may indirectly assist in clearing secretions, it does not directly address the issue of thinning the secretions, which is the primary concern in this scenario.
C. Prelubricate the suction catheter tip with sterile saline when suctioning the airway.
Prelubricating the suction catheter tip with sterile saline before suctioning can help reduce friction and potential trauma to the airway. While this can be beneficial for airway management, it does not directly address the need to thin copious and tenacious secretions.
D. Hyperventilate the client with 100% oxygen before suctioning the airway.
Hyperventilating the client with 100% oxygen before suctioning is not recommended. It can lead to respiratory alkalosis, which is a condition characterized by decreased levels of carbon dioxide in the blood. This can worsen the client's condition and may lead to adverse effects. Additionally, it does not directly address the need to thin secretions.
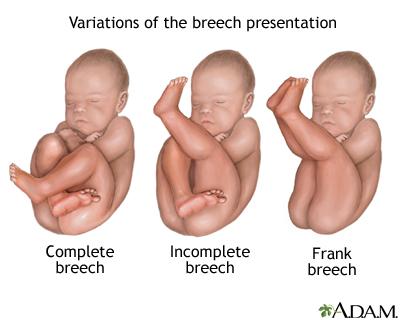
A nurse is caring for a client who is at 39 weeks of gestation and is in active labor. The nurse locates the fetal heart tones above the client's umbilicus at midline. The nurse should suspect that the fetus is in which of the following positions?
Explanation
Choice A rationale
This is correct because a frank breech position is when the fetus's buttocks are presenting at the cervix and the legs are extended upward toward the head. The fetal heart tones would be located above the umbilicus at midline, as the nurse observed.
Choice B rationale
This is incorrect because a cephalic position is when the fetus's head is presenting at the cervix and the body is aligned with the maternal spine. The fetal heart tones would be located below the umbilicus, either on the right or left side, depending on the fetal position.
Choice C rationale
This is incorrect because a posterior position is when the fetus's back is facing the maternal spine and the occiput is toward the sacrum. The fetal heart tones would be located below the umbilicus, either on the right or left side, depending on the fetal position.
Choice D rationale
This is incorrect because a transverse position is when the fetus's spine is perpendicular to the maternal spine and the shoulder is presenting at the cervix. The fetal heart tones would be located in the upper quadrants, either on the right or left side, depending on the fetal position.
A nurse is preparing to measure the fundal height of a client who is at 22 weeks of gestation. At which location should the nurse expect to palpate the fundus?
Explanation
Choice A rationale
This is incorrect because 3 cm above the umbilicus is not the expected location for the fundus at 22 weeks of gestation. The fundus is the upper part of the uterus that can be felt by abdominal palpation. The fundal height is measured from the symphysis pubis to the top of the fundus. The fundal height usually corresponds to the gestational age in weeks, plus or minus 2 cm. Therefore, at 22 weeks of gestation, the fundal height should be around 22 cm, which is slightly above the umbilicus.
Choice B rationale
This is incorrect because 3 cm below the umbilicus is not the expected location for the fundus at 22 weeks of gestation. The fundus is the upper part of the uterus that can be felt by abdominal palpation. The fundal height is measured from the symphysis pubis to the top of the fundus. The fundal height usually corresponds to the gestational age in weeks, plus or minus 2 cm. Therefore, at 22 weeks of gestation, the fundal height should be around 22 cm, which is slightly above the umbilicus.
Choice C rationale
This is incorrect because slightly below the umbilicus is not the expected location for the fundus at 22 weeks of gestation. The fundus is the upper part of the uterus that can be felt by abdominal palpation. The fundal height is measured from the symphysis pubis to the top of the fundus. The fundal height usually corresponds to the gestational age in weeks, plus or minus 2 cm. Therefore, at 22 weeks of gestation, the fundal height should be around 22 cm, which is slightly above the umbilicus.
Choice D rationale
This is correct because slightly above the umbilicus is the expected location for the fundus at 22 weeks of gestation. The fundus is the upper part of the uterus that can be felt by abdominal palpation. The fundal height is measured from the symphysis pubis to the top of the fundus. The fundal height usually corresponds to the gestational age in weeks, plus or minus 2 cm. Therefore, at 22 weeks of gestation, the fundal height should be around 22 cm, which is slightly above the umbilicus.
A nurse is leading a discussion about contraception with a group of 14-year-old clients. After the presentation, a client asks the nurse which method would be best for her to use. Which of the following responses should the nurse make?
Explanation
Choice A rationale
This is the most appropriate response because it emphasizes the importance of a healthcare provider's role in determining the best contraceptive method for an individual. It also respects the client's privacy and autonomy¹².
Choice B rationale
While it's important to understand a person's sexual activity when discussing contraception, asking for such details might make the client uncomfortable and could be seen as intrusive¹.
Choice C rationale
This response might be perceived as judgmental or patronizing. It's important to provide factual information and support without making assumptions about the client's readiness for a sexual relationship¹.
Choice D rationale
While barrier methods can be effective, they might not be the best choice for everyone. The best contraceptive method depends on a variety of factors, including the individual's health, lifestyle, and personal preferences¹². Therefore, it's best to consult with a healthcare provider¹².
A nurse in an antepartum unit is triaging clients. Which of the following clients should the nurse see first?
Explanation
Choice A rationale
This is incorrect because a client who has missed a period and reports vaginal spotting is not the most urgent case. This could indicate a possible pregnancy or a menstrual irregularity, but it is not a life-threatening condition. The nurse should see this client after assessing the other clients.
Choice B rationale
This is correct because a client who is at 28 weeks of gestation and reports painless vaginal bleeding is the most urgent case. This could indicate a placenta previa, which is a condition where the placenta covers the cervical opening and can cause severe hemorrhage and fetal distress. The nurse should see this client immediately and prepare for an emergency cesarean section.
Choice C rationale
This is incorrect because a client who is at 38 weeks of gestation and reports a cough and fever is not the most urgent case. This could indicate a respiratory infection, which can affect the maternal and fetal well-being, but it is not a life-threatening condition. The nurse should see this client after assessing the other clients and administer antibiotics and antipyretics as prescribed.
Choice D rationale
This is incorrect because a client who is at 14 weeks of gestation and reports nausea and vomiting is not the most urgent case. This could indicate a normal pregnancy symptom or a hyperemesis gravidarum, which is a condition where the nausea and vomiting are severe and persistent. The nurse should see this client after assessing the other clients and provide hydration and antiemetics as prescribed.
A nurse is assessing a client who is receiving magnesium sulfate to treat pre-eclampsia. Which of the following findings should the nurse report to the provider?
Explanation
Choice A rationale
This is incorrect because respirations 16/min are within the normal range and do not indicate magnesium toxicity. The nurse should monitor the client's respiratory rate and report any signs of respiratory depression, such as less than 12/min.
Choice B rationale
This is incorrect because fetal heart rate 158/min is within the normal range and does not indicate fetal distress. The nurse should monitor the fetal heart rate and report any signs of bradycardia, tachycardia, or decreased variability.
Choice C rationale
This is incorrect because headache for 30 min is a common symptom of pre-eclampsia and does not indicate magnesium toxicity. The nurse should administer analgesics as prescribed and report any signs of increased intracranial pressure, such as blurred vision, confusion, or seizures.
Choice D rationale
This is correct because urinary output 40 mL in 2 hr is below the expected amount and indicates renal impairment. The nurse should report this finding to the provider and monitor the client's fluid intake and output, serum creatinine, and blood urea nitrogen levels. The nurse should also assess the client for signs of fluid overload, such as edema, crackles, or dyspnea.
You just viewed 10 questions out of the 40 questions on the Ati Nurs 140 Proctored Exam Maternal Newborn Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

