
Pharmacology
ATI Pharmacology
Total Questions : 51
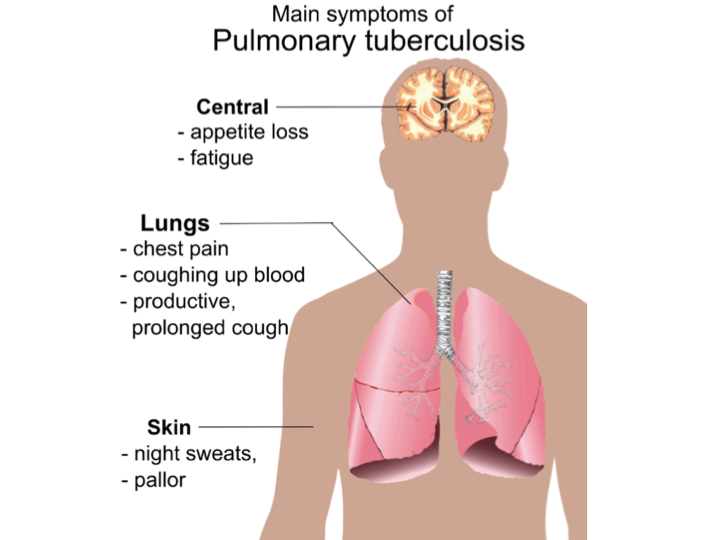
Showing 10 questions Sign up for moreA nurse in a provider’s office is assessing a client. The nurse should identify that which of the following findings are manifestations of pulmonary tuberculosis? (Select all that apply)
Explanation
Choice A reason: This is incorrect. Weight gain is not a manifestation of pulmonary tuberculosis. In fact, weight loss is a common symptom of tuberculosis, as the infection causes the body to use more energy and reduce appetite. Weight loss can also be a result of malnutrition, dehydration, or other complications of tuberculosis.
Choice B reason: This is correct. Night sweats are a manifestation of pulmonary tuberculosis. They occur because the infection causes the body to produce more heat and sweat to fight off the bacteria. Night sweats can also be a sign of fever, which is another symptom of tuberculosis.
Choice C reason: This is correct. Low-grade fever is a manifestation of pulmonary tuberculosis. It occurs because the infection causes the body to raise its temperature to kill the bacteria. Fever can also be accompanied by chills, fatigue, or weakness.
Choice D reason: This is correct. Blood in the sputum is a manifestation of pulmonary tuberculosis. It occurs because the infection causes damage and inflammation to the lungs and the airways, which can bleed and mix with the mucus that is coughed up. Blood in the sputum can also be a sign of a serious complication, such as a ruptured blood vessel or a lung abscess.
Choice E reason: This is incorrect. Flushed cheeks are not a manifestation of pulmonary tuberculosis. They can be caused by various factors, such as embarrassment, exercise, alcohol, or hot weather. Flushed cheeks are not related to the infection or the inflammation of the lungs.
A nurse is caring for a client who had a stroke involving the right cerebral hemisphere. The nurse should monitor for which of the following findings?
Explanation
Choice A reason: A stroke involving the right cerebral hemisphere can affect the cognitive and emotional functions of the brain, such as judgment, impulse control, and emotional regulation³. This can lead to risky or inappropriate behaviors, such as acting impulsively or disregarding social norms. Therefore, the nurse should monitor the client for poor impulse control and provide appropriate interventions, such as education, cueing, feedback, and environmental modifications.
Choice B reason: A stroke involving the right cerebral hemisphere can affect the visual functions of the brain, such as depth perception, spatial orientation, and visual recognition³. However, the deficits are usually in the left visual field, not the right, because the right side of the brain controls the left side of the body and the environment. Therefore, the nurse should monitor the client for deficits in the left visual field, not the right.
Choice C reason: A stroke involving the right cerebral hemisphere can affect the abstract reasoning functions of the brain, such as understanding metaphors, humor, or sarcasm. However, the ability to discriminate words and letters is more related to the language functions of the brain, which are mainly controlled by the left cerebral hemisphere. Therefore, the nurse should monitor the client for language deficits, such as aphasia or dysarthria, if the stroke involves the left cerebral hemisphere, not the right.
Choice D reason: A stroke involving the right cerebral hemisphere can affect the motor functions of the brain, such as movement, coordination, and balance³. However, the motor retardation, which is a slowing down of physical and mental activity, is more related to the mood functions of the brain, which are mainly controlled by the frontal lobe of the brain. Therefore, the nurse should monitor the client for motor retardation if the stroke involves the frontal lobe, not the right cerebral hemisphere.
A nurse is caring for a client who has a head injury. The client states they fell off a ladder while painting approximately 2 hours ago and lost consciousness for 45 minutes according to their partner. The nurse should determine that the client is experiencing which of the following classifications of traumatic brain injury?
Explanation
The correct answer is A. Moderate.
Choice A: Moderate
A moderate traumatic brain injury (TBI) is characterized by a loss of consciousness (LOC) lasting between 30 minutes and 6 hours. In this scenario, the client lost consciousness for 45 minutes, which falls within this range. Moderate TBIs often result in more significant symptoms and may require more intensive medical intervention compared to mild TBIs.
Choice B: Severe
Severe TBIs are typically defined by a loss of consciousness lasting more than 6 hours. Since the client in this case was unconscious for only 45 minutes, this classification does not apply. Severe TBIs often involve extensive brain damage and can lead to long-term complications or disabilities.
Choice C: Mild
Mild TBIs, also known as concussions, are characterized by a loss of consciousness lasting less than 30 minutes. Given that the client was unconscious for 45 minutes, this classification is not appropriate. Mild TBIs usually result in temporary symptoms that resolve with minimal medical intervention.
Choice D: No traumatic brain injury
This option is incorrect because the client experienced a significant head injury with a loss of consciousness for 45 minutes. Such an event clearly indicates a traumatic brain injury, and it is essential to classify it correctly to ensure appropriate medical care.
A nurse is planning care for a female client who has a T4 spinal cord injury and is at risk for acquiring urinary tract infections. Which of the following actions should the nurse include in the client’s plan of care?
Explanation
Choice A reason: This is incorrect. Cleansing the perineum from back to front can increase the risk of urinary tract infections, as it can introduce bacteria from the anal area to the urethra. The nurse should instruct the client to cleanse the perineum from front to back, using a mild soap and water, and to change the pad or underwear frequently to prevent bacterial growth.
Choice B reason: This is incorrect. Obtaining a prescription for an indwelling urinary catheter can increase the risk of urinary tract infections, as it can create a direct route for bacteria to enter the bladder. Indwelling catheters should be avoided unless absolutely necessary, and should be removed as soon as possible. The nurse should explore other bladder management options for the client, such as intermittent catheterization, condom catheter, or suprapubic catheter.
Choice C reason: This is incorrect. Offering the client the bedpan every 2 hours can increase the risk of urinary tract infections, as it can cause urinary stasis and bladder distension. The nurse should assess the client's bladder function and determine the optimal frequency of bladder emptying, which may vary depending on the type and level of spinal cord injury. The nurse should also monitor the client's urine output, color, odor, and clarity, and report any signs of infection, such as fever, chills, or flank pain.
Choice D reason: This is correct. Encouraging fluid intake at and between meals can decrease the risk of urinary tract infections, as it can flush out bacteria from the urinary tract and prevent urinary stasis and bladder distension. The nurse should advise the client to drink at least 2 liters of water per day, unless contraindicated by other medical conditions. The nurse should also educate the client about the benefits of cranberry juice, which can inhibit bacterial adhesion to the bladder wall and prevent infection.
A nurse is caring for a client who has had a stroke involving the right hemisphere. Which of the following alterations in function should the nurse expect?
Explanation
Choice A reason: This is incorrect. Right hemiparesis is not a common finding in clients who had a stroke involving the right hemisphere. Hemiparesis is the weakness or partial paralysis of one side of the body. It usually affects the opposite side of the body from the side of the brain that is damaged by the stroke. Therefore, a stroke in the right hemisphere would more likely cause left hemiparesis, not right hemiparesis.
Choice B reason: This is incorrect. Aphasia is not a common finding in clients who had a stroke involving the right hemisphere. Aphasia is the loss or impairment of language functions, such as speaking, understanding, reading, or writing. It usually affects the dominant hemisphere of the brain, which is the left hemisphere for most people. Therefore, a stroke in the right hemisphere would less likely cause aphasia, unless the person is lefthanded or ambidextrous.
Choice C reason: This is correct. Inability to recognize his family members is a common finding in clients who had a stroke involving the right hemisphere. This is a type of agnosia, which is the loss or impairment of the ability to recognize objects, people, sounds, shapes, or smells. The right hemisphere of the brain is responsible for processing visual and spatial information, as well as facial recognition. A stroke in this area can damage the ability to identify familiar faces, even those of close relatives or friends.
Choice D reason: This is incorrect. Difficulty reading is not a common finding in clients who had a stroke involving the right hemisphere. Reading is a language function that involves the recognition and comprehension of written words. It usually depends on the dominant hemisphere of the brain, which is the left hemisphere for most people. Therefore, a stroke in the right hemisphere would less likely cause difficulty reading, unless the person is lefthanded or ambidextrous.
A nurse is providing discharge teaching to a client who has pulmonary tuberculosis and a new prescription for rifampin. Which of the following information should the nurse provide?
Explanation
Choice A reason: This is incorrect. It is not best to take medication with meals. Rifampin is better absorbed when taken on an empty stomach, at least 1 hour before or 2 hours after a meal. Taking rifampin with food can reduce its effectiveness and increase the risk of drug resistance. The nurse should advise the client to take the medication as directed by the doctor, and to avoid foods that can interact with rifampin, such as cheese, yogurt, or alcohol.
Choice B reason: This is incorrect. Treatment with this medication will not last for 1 month. Rifampin is usually given as part of a combination therapy for pulmonary tuberculosis, along with other drugs such as isoniazid, pyrazinamide, and ethambutol. The standard treatment regimen for drug susceptible tuberculosis consists of an intensive phase of 2 months, followed by a continuation phase of 4 or 7 months, depending on the drug regimen and the patient's response. The nurse should inform the client about the duration and the importance of completing the full course of treatment, even if the symptoms improve or the tests become negative.
Choice C reason: This is incorrect. This medication does not cause insomnia. Rifampin does not affect the sleep cycle or the quality of sleep. However, rifampin can cause other side effects, such as nausea, vomiting, diarrhea, headache, or rash. The nurse should instruct the client to report any severe or persistent side effects to the doctor, and to avoid taking over-the-counter drugs or herbal supplements without consulting the doctor, as rifampin can interact with many other medications and reduce their effectiveness.
Choice D reason: This is correct. Urine and other secretions might turn orange. Rifampin can cause a harmless discoloration of body fluids, such as urine, saliva, sweat, tears, or breast milk. The color can range from orange to red or brown, depending on the concentration of the drug and the pH of the fluid. The nurse should reassure the client that this is a normal and expected effect of rifampin, and that it does not indicate any damage to the kidneys or other organs. The nurse should also warn the client that rifampin can stain contact lenses, dentures, or clothing, and advise the client to use disposable lenses, remove dentures before taking the drug, and wear dark colored clothes.
A nurse is providing discharge teaching to a client who has asthma and new prescriptions for cromolyn and albuterol, both by nebulizer. Which of the following statements by the client indicates an understanding of the teaching?
Explanation
Choice A reason: This is incorrect. Taking the albuterol before taking the cromolyn is not necessary. Albuterol and cromolyn are both used to treat asthma, but they have different mechanisms of action. Albuterol is a bronchodilator that relaxes the muscles around the airways and opens them up, making it easier to breathe. Cromolyn is a mast cell stabilizer that prevents the release of substances that cause inflammation and allergy symptoms in the airways. Albuterol is used to relieve acute asthma attacks, while cromolyn is used to prevent chronic asthma symptoms. The nurse should advise the client to use albuterol as needed for quick relief, and to use cromolyn regularly as prescribed to prevent asthma flareups.
Choice B reason: This is incorrect. Using both medications immediately after exercising is not recommended. Exercise can trigger asthma symptoms in some people, such as wheezing, coughing, or shortness of breath. This is called exercise induced bronchoconstriction (EIB) or exercise induced asthma (EIA). The nurse should advise the client to use albuterol 15 to 30 minutes before exercising to prevent EIB or EIA, and to avoid exercising in cold, dry, or polluted air. The nurse should also instruct the client to use cromolyn at least 15 minutes before exercising, as it takes time to work and does not provide immediate relief. The nurse should also tell the client to stop exercising and use albuterol if asthma symptoms occur during or after exercising.
Choice C reason: This is incorrect. Using cromolyn immediately if the breathing begins to feel tight is not effective. Cromolyn is not a rescue medication that can provide quick relief of asthma symptoms. It is a preventive medication that works by reducing the inflammation and sensitivity of the airways over time. The nurse should advise the client to use albuterol instead of cromolyn if the breathing begins to feel tight, as albuterol can rapidly open up the airways and ease the breathing. The nurse should also instruct the client to seek medical attention if the albuterol does not work or if the symptoms get worse.
Choice D reason: This is correct. Administering the medications 10 minutes apart is good practice. Cromolyn and albuterol can be used together to treat asthma, but they should not be mixed in the same nebulizer, as they may not be compatible and may lose their effectiveness. The nurse should instruct the client to use separate nebulizers for each medication, and to wait at least 10 minutes between each nebulization to allow the medication to reach the lungs and avoid irritation of the airways. The nurse should also teach the client how to use the nebulizer properly, and how to clean and store it after each use.

A nurse is assessing a client who is 1 day postoperative following a lobectomy and has a chest tube drainage system in place. Which of the following findings by the nurse indicates a need for intervention?
Explanation
The correct answer is: a. Development of subcutaneous emphysema
Choice A: Development of subcutaneous emphysema
Reason: Subcutaneous emphysema occurs when air gets trapped under the skin, often due to a leak from the lung or chest tube. This can indicate a serious complication such as a pneumothorax or a malfunctioning chest tube, requiring immediate medical intervention. The presence of subcutaneous emphysema can lead to discomfort, respiratory distress, and further complications if not addressed promptly.
Choice B: Chest tube eyelets not visible
Reason: The eyelets of a chest tube are small holes at the end of the tube that allow air and fluid to drain from the pleural space. These eyelets are typically covered by a dressing and may not be visible. This is not necessarily a cause for concern unless there are other signs of malfunction or complications.
Choice C: Continuous bubbling in the suction control chamber
Reason: Continuous bubbling in the suction control chamber is expected and indicates that the suction is functioning properly. It does not indicate a problem unless the bubbling is in the water seal chamber, which would suggest an air leak.
Choice D: Presence of tidal fluctuation in the water seal chamber
Reason: Tidal fluctuation, or tidaling, in the water seal chamber is a normal finding. It indicates that the chest tube is patent and functioning correctly, as the water level rises with inhalation and falls with exhalation. The absence of tidaling could indicate a blockage or that the lung has fully re-expanded.
A nurse is caring for a child who is experiencing status asthmaticus. Which of the following interventions is the priority for the nurse to take?
Explanation
Choice A reason: Administering an inhaled glucocorticoid is not the priority intervention for a child with status asthmaticus. Inhaled glucocorticoids are anti-inflammatory drugs that reduce airway inflammation and prevent asthma attacks, but they do not provide immediate relief of bronchoconstriction.
Choice B reason: Administering a short acting beta agonist (SABA) is the priority intervention for a child with status asthmaticus. SABAs are bronchodilators that relax the smooth muscles of the airways and improve airflow within minutes. They are the first line treatment for acute asthma symptoms and exacerbations.
Choice C reason: Determining the cause of the acute exacerbation is not the priority intervention for a child with status asthmaticus. While it is important to identify and avoid potential triggers of asthma, such as allergens, infections, or stress, this is not an urgent action during a severe asthma attack.
Choice D reason: Obtaining a peak flow reading is not the priority intervention for a child with status asthmaticus. Peak flow is a measure of how quickly the child can blow air out of the lungs, and it can indicate the degree of airway obstruction. However, peak flow measurement is not reliable or feasible during a severe asthma attack, and it should not delay the administration of bronchodilators.
A nurse is caring for a client who has a three-chamber closed chest tube system. Which of the following actions should the nurse take after noticing a rise in the water seal chamber with client inspiration?
Explanation
Choice A reason: Repositioning the client toward the left side is not necessary or helpful for a client who has a three-chamber closed chest tube system. The chest tube drainage system must always be placed below the drainage site and secured in an upright position to prevent it from being knocked over.
Choice B reason: Continuing to monitor the client is the appropriate action for the nurse to take after noticing a rise in the water seal chamber with client inspiration. The water in the water seal chamber should rise with inhalation and fall with exhalation (this is called tidaling), which demonstrates that the chest tube is patent. This is a normal finding and does not indicate a problem with the chest tube system or the client's condition.
Choice C reason: Clamping the chest tube near the water seal is not recommended for a client who has a three-chamber closed chest tube system. Clamping the chest tube can cause a buildup of air or fluid in the pleural space and increase the risk of complications such as tension pneumothorax or infection. Clamping the chest tube should only be done in certain situations, such as changing the drainage system, checking for an air leak, or removing the chest tube.
Choice D reason: Immediately notifying the provider is not necessary for a client who has a three-chamber closed chest tube system and shows a rise in the water seal chamber with client inspiration. As mentioned above, this is a normal finding and does not indicate a problem with the chest tube system or the client's condition. The nurse should only notify the provider if there are signs of complications, such as continuous bubbling in the water seal chamber, excessive drainage, chest pain, dyspnea, or subcutaneous emphysema.
You just viewed 10 questions out of the 51 questions on the ATI Pharmacology Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

