
RN Ati fundamental of nursing proctored exam
RN Ati fundamental of nursing proctored exam
Total Questions : 68
Showing 10 questions Sign up for moreA nurse is preparing to administer a cleansing enema to a client. Which of the following actions should the nurse take?
Explanation
A. This is the appropriate height to allow the fluid flow by gravity.
B. This is such a short distance and the fluid wouldn't flow as desired.
C. Holding the container at the client's upper hip would not provide the appropriate angle for administering the enema.
D. This choice does not provide specific guidance on the height or angle for administering the enema, which is crucial for the procedure's effectiveness.
A nurse is assisting with transferring a client from the bed to a wheelchair. Which of the following actions should the nurse take?
Explanation
A. Elevating the bed for the comfort of the nurse does not address the safety and comfort of the client during the transfer.
B. While it's important to have assistance if needed, using several people to lift the client may not always be necessary or appropriate.
C. This positioningis not optimal, as it makes it harder for the client to pivot and sit on the wheelchair.
D. Ensuring the wheels of both the bed and the wheelchair are locked helps maintain stability and safety during the transfer process, reducing the risk of accidental movement and potential falls.
A nurse in a long-term care facility is caring for an older adult client who has dementia and begins to have frequent episodes of urinary incontinence. After the provider determines no medical cause for the client's incontinence, which of the following interventions should the nurse initiate to manage this behavior?
Explanation
A. Using an indwelling urinary catheter should be avoided unless absolutely necessary due to the associated risks of infection and other complications. It's not the first-line intervention for managing urinary incontinence.
B. Frequent toileting, also known as scheduled toileting or prompted voiding, is an effective intervention for managing urinary incontinence in older adults with dementia. It helps prevent accidents by ensuring the client has regular opportunities to use the
bathroom.
C. Reminding the client to tell the nurse when they need to urinate can be helpful, but it may not be sufficient on its own, especially for individuals with dementia who may have difficulty recognizing or communicating their needs.
D. Using adult diapers should be considered a last resort, as it does not address the underlying issue and may not promote the client's independence or dignity.
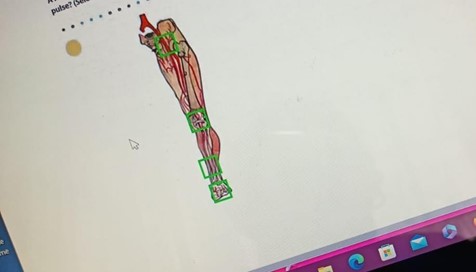
A nurse is assessing a client's peripheral circulation. In which of the following locations should the nurse palpate to assess the posterior tibial pulse? (Selectable areas, or "Hot Spots," are outlined in the artwork below. Select only the outlined area that corresponds to your answer.)
Explanation
A. Inguinal canal is not the correct location for assessing the posterior tibial pulse. This area is associated with the femoral pulse.
B. The knee is not the correct location for assessing the posterior tibial pulse. This area is not directly related to the posterior tibial pulse.
C. The lower third of the tibia, anterior aspect is the correct location for palpating the posterior tibial pulse. This pulse can be found on the inside of the ankle, slightly below and behind the medial malleolus.
D. Dorsal aspect of the foot is where the dorsalis pedis pulse is located, not the posterior tibial pulse.
A nurse is assessing a client's cranial nerves as part of a neurological examination. Which of the following actions should the nurse take to assess cranial nerve III?
Explanation
A. Cranial nerve III, also known as the oculomotor nerve, controls the muscles that move the eye and regulates the size of the pupil. Assessing the pupillary response to light helps evaluate the function of this nerve.
B. Eliciting the gag reflex is associated with cranial nerves IX (glossopharyngeal) and X (vagus), not cranial nerve III.
C. Testing visual acuity is primarily associated with cranial nerve II (optic nerve), not cranial nerve III.
D. Observing facial symmetry is important for assessing cranial nerve VII (facial nerve), not cranial nerve III.
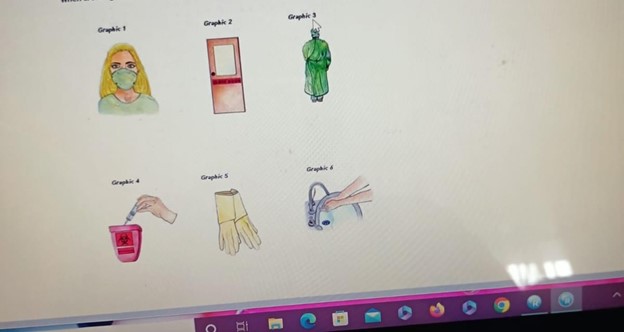
A nurse is caring for a client who requires isolation for active pulmonary tuberculosis. Which of the following precautions should the nurse include when creating a sign to post outside of the client's room? (Select all that apply.)
Explanation
A. Wearing a mask helps protect against the transmission of airborne particles, which is important for preventing the spread of tuberculosis.
B. Wearing a gown can provide an additional barrier to prevent the transmission of infectious material.
C. Disposing sharps here is not directly related to tuberculosis precautions. This statement is more relevant for a sharps disposal container.
D. Wearing gloves is important to prevent direct contact with potentially contaminated surfaces.
E. Hand hygiene is crucial for infection control and should be emphasized for anyone entering or exiting the room of a client in isolation.
F. "Radiation inside" is not applicable to the isolation precautions for tuberculosis. This statement is unrelated to tuberculosis precautions and may cause confusion.
A nurse is assisting with transferring a client from the bed to a wheelchair. Which of the following actions should the nurse take?
Explanation
- A) Elevating the bed to a comfortable position for the nurse is important to prevent strain or injury to the nurse's back. However, this action alone does not ensure the client's safety during the transfer.
- B) While acquiring help can be useful, especially for a heavy client or one with limited mobility, it is not the primary action to ensure safety during the transfer.
- C) Placing the wheelchair at a 90° angle to the bed may make the transfer more difficult because it does not allow for the most direct path to the wheelchair.
- D) Locking the wheels of both the bed and the wheelchair is the correct action to take to ensure stability and prevent movement, providing a safe transfer for the client.
A nurse is reviewing information about the Health Insurance Portability and Accountability Act (HIPAA) with a newly licensed nurse. Which of the following statements by the newly licensed nurse indicates a need for further teaching?
Explanation
A. This statement is incorrect. While HIPAA allows for certain disclosures to family members, it is important to follow specific guidelines and obtain appropriate consent or authorization from the client when sharing their health information. There are also circumstances where a client may request that information be withheld from certain family members.
B. This statement is correct. HIPAA is a federal law that establishes privacy standards for protected health information.
C. This statement is correct. A client's address is considered personally identifiable information under HIPAA.
D. The statement appears to be cut off. However, it is important to note that HIPAA does indeed establish regulations for protecting individually identifiable health information in various forms, including verbal, electronic, and written.
A nurse removes an indwelling urinary catheter that an older adult client has had in place for 2 days. The nurse should assess the client for which of the following expected outcomes after catheter removal?
Explanation
A. After removal of an indwelling urinary catheter, it is common for a client to experience urinary frequency for a few days. This is due to the bladder readjusting to its normal function.
B. Blood-tinged urine may occur after catheter removal, but it is not an expected outcome. It should be assessed and reported if it occurs.
C. Highly concentrated urine is not typically an expected outcome after catheter removal.
It may indicate dehydration or another issue that should be addressed.
D. Temporary urinary retention can occur after catheter removal, especially in older adults. This is why it's important to monitor the client for signs of retention, such as discomfort, restlessness, or a palpable bladder.
A nurse is caring for a client who has a wound infection. Which of the following actions should the nurse take when obtaining a wound-drainage specimen for culture?
Explanation
A. Irrigating the wound with an antiseptic prior to obtaining the specimen can introduce substances that may interfere with the accuracy of the culture results. Sterile saline is the preferred solution for wound irrigation.
B. Intact skin at the wound edges should not be included in the culture. The specimen should be obtained directly from the wound bed or drainage.
C. Swabbing an area of skin away from the wound to identify the usual flora is not appropriate for obtaining a wound drainage specimen. The culture should be taken directly from the wound site.
D. Before obtaining a wound-drainage specimen for culture, it is important to cleanse the wound with a sterile solution, such as 0.9% sodium chloride saline irrigation. This helps remove debris and contaminants from the wound site, providing a more accurate specimen for culture.
You just viewed 10 questions out of the 68 questions on the RN Ati fundamental of nursing proctored exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

