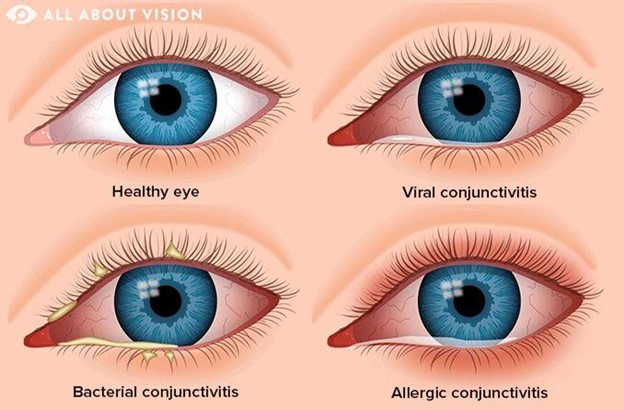
A client arrives with a pink eye that is itchy, swollen, and uncomfortable with a creamy discharge. Which of the following home care instructions will the nurse offer to the client?
Wash towels, sheets, and pillowcases
Use antifungal drops 3 times a day
Schedule a sexually transmitted infection (STI/STD) exam
Avoid going outside during daylight hours
The Correct Answer is A
Choice A Reason: This is the correct choice. Washing towels, sheets, and pillowcases is a home care instruction that the nurse will offer to the client, as it prevents reinfection and transmission of bacteria or viruses. The client has conjunctivitis, which is inflammation of the conjunctiva or thin membrane that covers the white part of the eye and lines the eyelids. It can be caused by bacteria, viruses, allergies, or irritants.
Choice B Reason: This is an incorrect choice. Using antifungal drops 3 times a day is not a home care instruction that the nurse will offer to the client, as it is not effective for conjunctivitis. Antifungal drops are used for fungal infections of the eye, which are rare and usually occur after trauma or surgery. The client may need antibiotic or antiviral drops, depending on the cause of conjunctivitis.
Choice C Reason: This is an incorrect choice. Scheduling a sexually transmitted infection (STI/STD) exam is not a home care instruction that the nurse will offer to the client, as it is not relevant for conjunctivitis. STIs can affect the eyes, but they usually cause different symptoms, such as redness, pain, or discharge from the urethra or vagina. The client may need to be tested for STIs if they have other risk factors or signs of infection.
Choice D Reason: This is an incorrect choice. Avoiding going outside during daylight hours is not a home care instruction that the nurse will offer to the client, as it is not necessary for conjunctivitis. The client may experience sensitivity to light, but they can wear sunglasses or avoid direct sunlight to protect their eyes. The client should also avoid rubbing or touching their eyes, wear glasses instead of contact lenses, and discard any eye makeup or cosmetics that may be contaminated.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because drawing with crayons may be too childish or frustrating for a client with moderate Alzheimer's. Crayons may also pose a choking hazard or cause messes. The nurse should provide activities that are suitable for the client's cognitive and functional level, as well as their interests and preferences.
Choice B Reason: This is incorrect because dangling ribbons or a mobile may be too stimulating or confusing for a client with moderate Alzheimer's. These items may also trigger agitation or wandering behaviors. The nurse should provide activities that are calming and familiar for the client.
Choice C Reason: This is correct because listening to music, watching TV, or videos can be enjoyable and beneficial for a client with moderate Alzheimer's. Music can evoke memories, emotions, and positive responses. TV or videos can provide entertainment, education, and socialization. The nurse should choose music, TV shows, or videos that are appropriate and meaningful for the client.
Choice D Reason: This is incorrect because board games may be too complex or challenging for a client with moderate Alzheimer's. Board games may require memory, concentration, logic, or strategy skills that the client may have lost. The nurse should provide activities that are simple and easy for the client to follow.
Correct Answer is ["B","E","F"]
Explanation
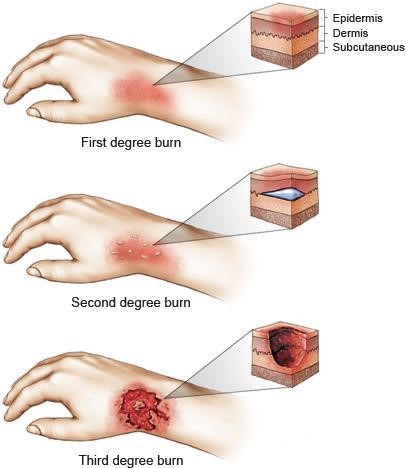
Choice A Reason: This is incorrect because submerging the client in a cold bath can cause hypothermia, shock, or infection. Cold water can lower the body temperature and blood pressure, which can impair circulation and organ function. Cold water can also introduce bacteria or contaminants into the open wounds. The nurse should use cool water or saline to gently irrigate the burned areas and then cover them with sterile dressings.
Choice B Reason: This is correct because administering oxygen can help the client breathe better and prevent hypoxia. Burns to the face, neck, or chest can cause swelling or damage to the airway, which can impair gas exchange and oxygen delivery. Oxygen can also reduce the risk of carbon monoxide poisoning, which can occur from inhaling smoke or fumes.
Choice C Reason: This is incorrect because restricting fluids can worsen dehydration and shock. Burns can cause significant fluid and electrolyte loss through evaporation and leakage from damaged capillaries. This can lead to hypovolemia, which is low blood volume, and hypotension, which is low blood pressure. The nurse should monitor the client's vital signs, urine output, and weight, and administer intravenous fluids as ordered.
Choice D Reason: This is incorrect because providing a meal high in fiber can cause abdominal discomfort or diarrhea. Burns can cause paralytic ileus, which is a temporary loss of bowel function due to nerve damage or inflammation. This can impair digestion and absorption of food and cause nausea, vomiting, or constipation. The nurse should assess the client's bowel sounds and provide enteral or parenteral nutrition as ordered.
Choice E Reason: This is correct because assessing airway is a priority nursing action for a client with burns. As mentioned above, burns to the face, neck, or chest can compromise the airway and cause respiratory distress or failure. The nurse should assess the client's level of consciousness, breathing rate and pattern, oxygen saturation, and signs of inhalation injury, such as sooty sputum, singed nasal hairs, or hoarseness. The nurse should also be prepared to assist with intubation or tracheostomy if needed.
Choice F Reason: This is correct because applying ice to burned areas can help reduce pain and swelling. Ice can constrict blood vessels and numb nerve endings, which can decrease inflammation and sensation. However, ice should be applied for no more than 15 minutes at a time and wrapped in a cloth or towel to prevent frostbite or tissue damage. Ice should not be applied to large or deep burns.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today