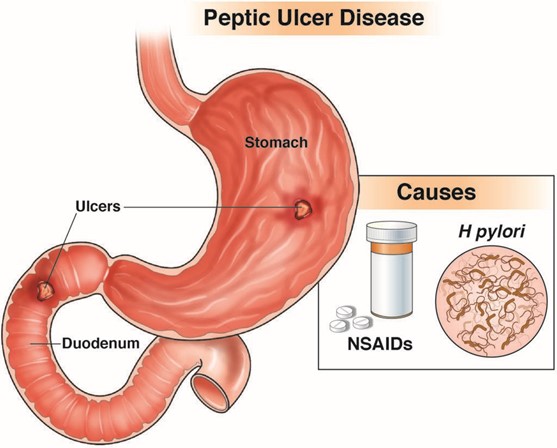
A client was admitted in the hospital with peptic ulcer disease tells the nurse about having black tarry stools. Which of the following is the most appropriate nursing action?
Instruct the client to increase fluid intake.
Notify the health care provider.
Advise the client to take iron rich foods.
Document the findings.
The Correct Answer is B
Choice A Reason: Instructing the client to increase fluid intake is not the most appropriate nursing action, as it does not address the cause or severity of the bleeding.
Choice B Reason: Notifying the health care provider is the most appropriate nursing action, as it indicates that the client may have a bleeding ulcer that requires immediate evaluation and treatment.
Choice C Reason: Advising the client to take iron rich foods is not the most appropriate nursing action, as it does not prevent or correct anemia or bleeding.
Choice D Reason: Documenting the findings is not the most appropriate nursing action, as it does not initiate any intervention or outcome.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: Murphy sign is a finding that indicates cholecystitis, which is inflammation of the gallbladder. It is elicited by palpating the right upper quadrant of the abdomen and asking the client to take a deep breath. The client will experience pain and stop breathing in if cholecystitis is present.
Choice B Reason: McBurney sign is a finding that indicates appendicitis, which is inflammation of the appendix. It is elicited by palpating the right lower quadrant of the abdomen at a point one-third of the distance from the anterior superior iliac spine to the umbilicus. The client will experience pain and tenderness if appendicitis is present.
Choice C Reason: Cullen's sign is a finding that indicates intra-abdominal bleeding, which can be caused by various conditions such as ruptured ectopic pregnancy, pancreatitis, or trauma. It is characterized by bruising around the umbilicus due to blood accumulation under the skin.
Choice D Reason: Homan sign is a finding that indicates deep vein thrombosis (DVT), which is a blood clot in a deep vein, usually in the leg. It is elicited by dorsiflexing the foot and squeezing the calf muscle. The client will experience pain and resistance if DVT is present.
Correct Answer is B
Explanation
Choice A Reason: Painful urination is not a common finding in BPH, but it may indicate a urinary tract infection or bladder stones.
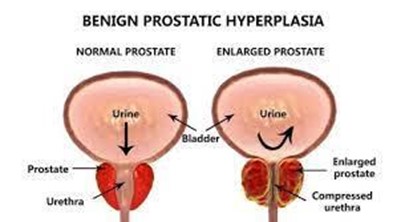
Choice B Reason: Decreased urinary stream is a common finding in BPH, as the enlarged prostate compresses the urethra and obstructs the flow of urine.
Choice C Reason: Critically elevated PSA level is not a common finding in BPH, but it may indicate prostate cancer or prostatitis.
Choice D Reason: Urge incontinence is not a common finding in BPH, but it may indicate an overactive bladder or neurogenic bladder.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today