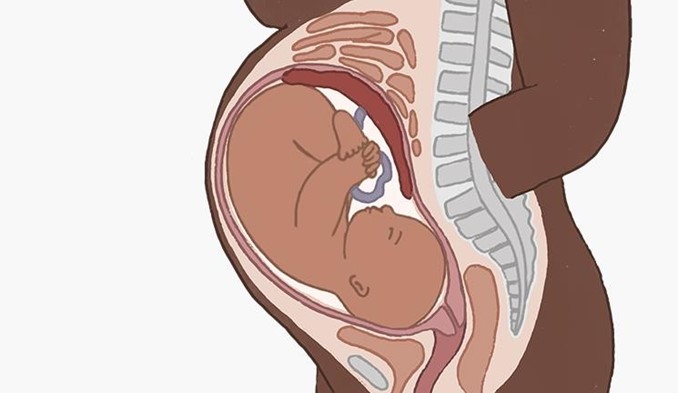
A nurse in a hospital is caring for a client who is at 38 weeks of gestation and has a large amount of painless, bright red vaginal bleeding. The client is placed on a fetal monitor indicating a regular fetal heart rate of 138/min and no uterine contractions. The client's vital signs are: blood pressure 98/52 mm Hg, heart rate 118/min, respiratory rate 24/min, and temperature 36.4°C (97.6°F). Which of the following is the priority nursing action?
Insert an indwelling urinary catheter.
Prepare the abdominal and perineal areas.
Witness the signature for informed consent for surgery.
Initiate IV access.
The Correct Answer is D
Choice a) Insert an indwelling urinary catheter is incorrect because this is not a priority action for a client who has a large amount of painless, bright red vaginal bleeding. This type of bleeding is suggestive of placenta previa, which is a condition where the placenta covers part or all of the cervix, preventing normal delivery. Inserting an indwelling urinary catheter can cause trauma to the cervix or the placenta, which can worsen the bleeding and endanger the mother and the fetus. Therefore, this action should be avoided unless absolutely necessary.
Choice b) Prepare the abdominal and perineal areas is incorrect because this is not a priority action for a client who has a large amount of painless, bright red vaginal bleeding. This type of bleeding is suggestive of placenta previa, which is a condition where the placenta covers part or all of the cervix, preventing normal delivery. Preparing the abdominal and perineal areas can be done before performing a cesarean section, which is usually the preferred mode of delivery for placenta previa. However, this action should be done after stabilizing the client's condition and obtaining informed consent for surgery.
Choice c) Witness the signature for informed consent for surgery is incorrect because this is not a priority action for a client who has a large amount of painless, bright red vaginal bleeding. This type of bleeding is suggestive of placenta previa, which is a condition where the placenta covers part or all of the cervix, preventing normal delivery.
Witnessing the signature for informed consent for surgery can be done before performing a cesarean section, which is usually the preferred mode of delivery for placenta previa. However, this action should be done after stabilizing the client's condition and explaining the risks and benefits of surgery.
Choice d) Initiate IV access is correct because this is the priority action for a client who has a large amount of painless, bright red vaginal bleeding. This type of bleeding is suggestive of placenta previa, which is a condition where the placenta covers part or all of the cervix, preventing normal delivery. Initiating IV access can help to restore fluid volume, prevent hypovolemic shock, administer medications such as oxytocin or blood products if needed, and prepare for emergency cesarean section if indicated. Therefore, this action should be done as soon as possible to save the life of the mother and the fetus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
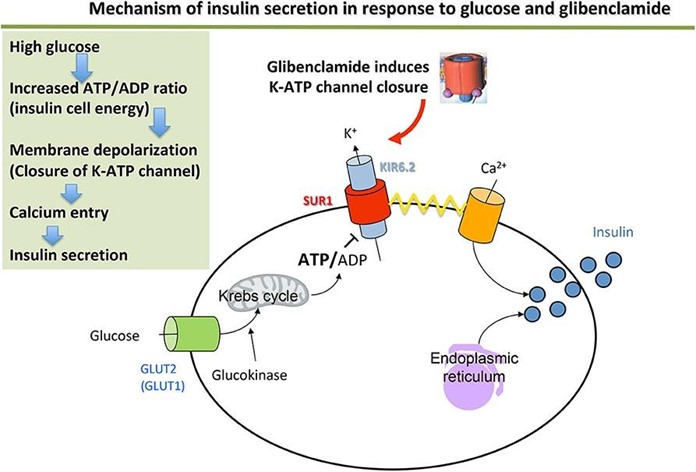
Choice a) Document the event in the nurses' notes is incorrect because this is not a priority action for a neonate who is showing signs of hypoglycemia. Hypoglycemia is a condition where the blood glucose level is lower than normal, which can cause neurological and metabolic problems in newborns. Neonates of diabetic mothers are at higher risk of developing hypoglycemia due to increased insulin production and decreased glycogen stores.
Documenting the event in the nurses' notes is an important step, but it should be done after assessing and treating the neonate's condition.
Choice b) Test for blood glucose level is correct because this is the most important action for a neonate who is exhibiting symptoms of hypoglycemia. The nurse should use a heel stick or a cord blood sample to measure the blood glucose level of the neonate as soon as possible, as hypoglycemia can lead to serious complications such as seizures, coma, brain damage, or death if left untreated. The normal blood glucose range for a full-term neonate is 40 to 60 mg/dL in the first hour of life, and 50 to 90 mg/dL thereafter. A blood glucose level below 40 mg/dL indicates hypoglycemia and requires immediate intervention.
Choice c) Notify the clinician stat is incorrect because this is not the most urgent action for a neonate who is suffering from hypoglycemia. The nurse should notify the clinician after confirming the diagnosis of hypoglycemia and initiating treatment, such as feeding or administering intravenous glucose. The clinician may order further tests or treatments depending on the severity and cause of the hypoglycemia, but the nurse should not delay the initial management of the neonate's condition.
Choice d) Start an intravenous line with D5W is incorrect because this is not the first-line treatment for a neonate who has hypoglycemia. D5W stands for dextrose 5% in water, which is a solution that contains glucose and water. It can be used to treat hypoglycemia by providing a source of energy and fluid to the neonate. However, before starting an intravenous line with D5W, the nurse should first attempt to feed the neonate with breast milk or formula, as this can also raise the blood glucose level and provide other nutrients and antibodies. If feeding is unsuccessful or contraindicated, then the nurse should start an intravenous line with D5W as ordered by the clinician.
Correct Answer is A
Explanation
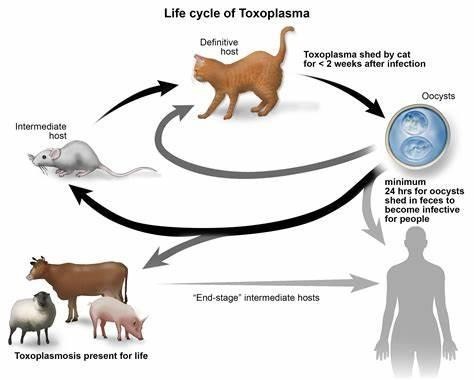
Choice a) I will be certain to empty the litter boxes regularly is incorrect because this is a risky behavior for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis is an infection caused by a parasite called Toxoplasma gondii, which can be found in the feces of cats and other animals. If a pregnant woman gets infected with toxoplasmosis, she can pass it to her unborn baby, which can cause serious problems such as miscarriage, stillbirth, or birth defects. Therefore, a pregnant woman should avoid contact with cat litter and let someone else handle the litter boxes, or wear gloves and wash her hands thoroughly if she has to do it herself.
Choice b) I have to wash all of my fruits and vegetables is correct because this is a good practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be transmitted through contaminated soil or water, which can adhere to fruits and vegetables. Therefore, a pregnant woman should wash all of her fruits and vegetables before eating them, and peel or cook them if possible, to remove any traces of the parasite.
Choice c) I won't eat raw eggs is correct because this is another good practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be acquired through eating undercooked or raw meat or eggs that contain the parasite. Therefore, a pregnant woman should avoid eating raw eggs or any foods that contain them, such as mayonnaise, mousse, or homemade ice cream, and cook all of her meat and eggs thoroughly until they are no longer pink or runny.
Choice d) I need to be cautious when cooking meat is correct because this is also an important practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be spread through handling raw meat that contains the parasite. Therefore, a pregnant woman should be careful when cooking meat and use separate utensils and cutting boards for raw and cooked meat, wash her hands and surfaces after touching raw meat, and avoid tasting raw meat while cooking it.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today