Which of the following would the nurse expect to assess in a newborn who develops sepsis?
Increased urinary output
Hypothermia
Wakefulness
Interest in feeding
The Correct Answer is B
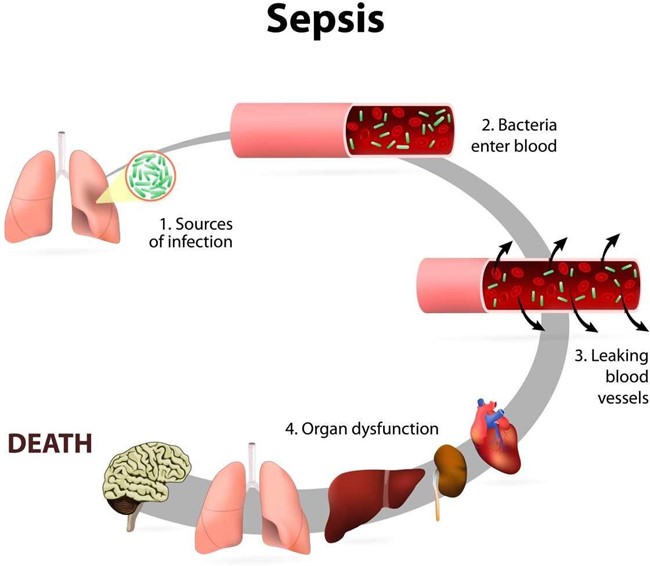
Choice A) Increased urinary output: This is not a sign of sepsis in newborns. In fact, sepsis can cause reduced urinary output due to poor blood flow to the kidneys and dehydration.
Choice B) Hypothermia: This is a sign of sepsis in newborns. Sepsis can cause changes in temperature, often fever, but sometimes low temperature. Hypothermia can indicate a severe infection that affects the body's ability to regulate its temperature.
Choice C) Wakefulness: This is not a sign of sepsis in newborns. Sepsis can cause reduced activity and lethargy due to inflammation and organ dysfunction.
Choice D) Interest in feeding: This is not a sign of sepsis in newborns. Sepsis can cause reduced sucking and difficulty feeding due to poor appetite, nausea, vomiting, and abdominal distension.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
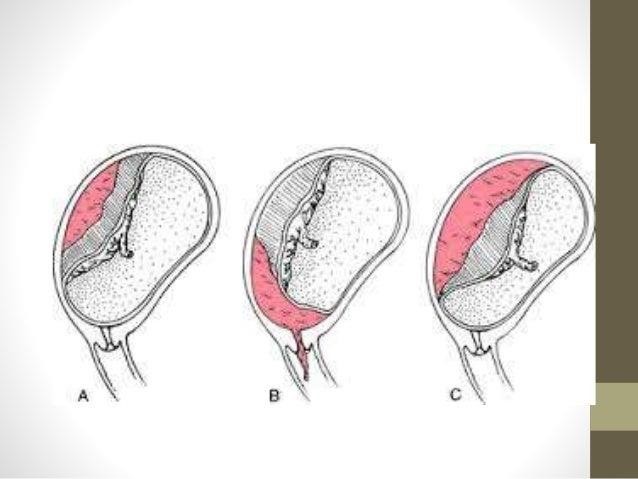
Choice a) This could result in profound bleeding is correct because this is the primary reason why an internal examination should be avoided for a client who has placenta previa. Placenta previa is a condition where the placenta covers part or all of the cervix, preventing normal delivery. An internal examination involves inserting a gloved finger or a speculum into the vagina and cervix to assess their dilation, effacement, position, and station. This can cause trauma to the cervix or the placenta, which can trigger severe hemorrhage and endanger the mother and the fetus. Therefore, this explanation is accurate and appropriate.
Choice b) This could initiate preterm labor is incorrect because this is not the main reason why an internal examination should be avoided for a client who has placenta previa. Placenta previa is a condition where the placenta covers part or all of the cervix, preventing normal delivery. An internal examination may stimulate uterine contractions, which can lead to preterm labor and delivery. However, this is not the most serious or likely complication of an internal examination for a client who has placenta previa, as the bleeding risk is much higher and more urgent. Therefore, this explanation is incomplete and misleading.
Choice c) There is an increased risk of introducing infection is incorrect because this is not a specific reason why an internal examination should be avoided for a client who has placenta previa. Placenta previa is a condition where the placenta covers part or all of the cervix, preventing normal delivery. An internal examination may introduce bacteria or other microorganisms into the vagina or cervix, which can cause infection and inflammation. However, this is a general risk that applies to any pregnant woman who undergoes an internal examination, not just those who have placenta previa. Therefore, this explanation is irrelevant and inaccurate.
Choice d) There is an increased risk of rupture of the membranes is incorrect because this is not a relevant reason why an internal examination should be avoided for a client who has placenta previa. Placenta previa is a condition where the placenta covers part or all of the cervix, preventing normal delivery. An internal examination may cause rupture of the membranes, which are the sacs that contain the amniotic fluid and the fetus. However, this is not a significant or common complication of an internal examination for a client who has placenta previa, as the membranes are usually located above or away from the placenta and cervix. Therefore, this explanation is improbable and inaccurate.
Correct Answer is C
Explanation
Choice A: This is incorrect because preeclampsia is a condition characterized by hypertension, proteinuria, and edema that occurs after 20 weeks of gestation. It is not related to abruptio placentae, which is the premature separation of the placenta from the uterine wall. Preeclampsia does not cause petechiae or bleeding around the IV site, but it may cause headache, blurred vision, epigastric pain, or seizures.
Choice B: This is incorrect because anaphylactoid syndrome of pregnancy, also known as amniotic fluid embolism, is a rare and life-threatening complication that occurs when amniotic fluid enters the maternal circulation and triggers an allergic reaction. It is not related to abruptio placentae, but it may occur during labor, delivery, or shortly after birth. Anaphylactoid syndrome of pregnancy does not cause petechiae or bleeding around the IV site, but it may cause respiratory distress, hypotension, cardiac arrest, or disseminated intravascular coagulation.
Choice C: This is the correct answer because disseminated intravascular coagulation (DIC) is a condition in which the blood clotting system is activated abnormally, leading to excessive clot formation and consumption of clotting factors and platelets. This results in bleeding from various sites, such as the IV site, gums, nose, or vagina. DIC is a common complication of abruptio placentae, as the release of thromboplastin from the placenta triggers the clotting cascade. DIC can also cause organ failure, shock, or death if not treated promptly.
Choice D: This is incorrect because puerperal infection, also known as postpartum infection, is a bacterial infection that affects the uterus, vagina, bladder, or wound site after childbirth. It is not related to abruptio placentae, but it may occur due to prolonged labor, cesarean delivery, retained placenta, or poor hygiene. Puerperal infection does not cause petechiae or bleeding around the IV site, but it may cause fever, malaise, foul-smelling lochia, or pelvic pain.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today