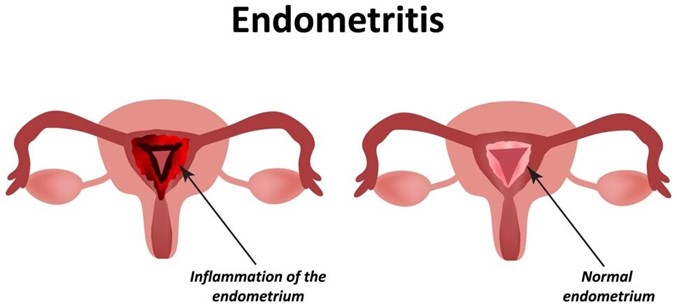
A nurse is assessing a client who is 6 hours postpartum and has endometritis. Which of the following findings should the nurse expect?
Temperature 37.4°C (99.3°F)
Scant lochia
Uterine tenderness
WBC count 9,000/mm³
The Correct Answer is C
Endometritis is an infection of the endometrium, the lining of the uterus, typically occurring after childbirth. When assessing a client with endometritis, the nurse should expect to find uterine tenderness as a common clinical finding. This finding is consistent with endometritis, which is characterized by inflammation and infection of the endometrium. Additional signs and symptoms may include an elevated temperature, increased lochia, foul-smelling lochia, and an elevated WBC count. Prompt identification and treatment of endometritis are important to prevent further complications.
Option a) A temperature of 37.4°C (99.3°F) is within the normal range and does not necessarily indicate endometritis. However, an elevated temperature above 38°C (100.4°F) or a persistent fever may be indicative of an infection and should be further evaluated.
Option b) Scant lochia (minimal vaginal bleeding) is not a characteristic finding of endometritis. In endometritis, lochia is often increased in amount and may have an unpleasant odor.
Option d) A white blood cell (WBC) count of 9,000/mm³ is within the normal range. However, in cases of endometritis, there is usually an elevation in the WBC count as a response to the infection. An elevated or increasing WBC count may be observed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
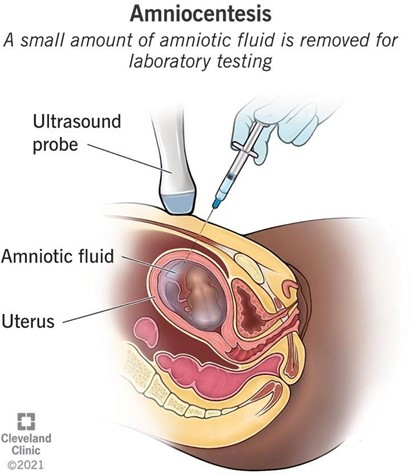
This is because a prescription for an amniocentesis is an indication for the administration of Rho(D) immune globulin (RhIG) to prevent RhD isoimmunization in mothers who are RhD negative¹². RhD isoimmunization is a condition where the mother's immune system produces antibodies against the RhD antigen on the baby's red blood cells, which can cause hemolytic disease of the newborn (HDN)¹². RhIG is a medication that contains antibodies against the RhD antigen, and it works by binding to and destroying any fetal red blood cells that may enter the maternal circulation, preventing the mother from making her own antibodies¹²³. RhIG is usually given to RhD negative mothers during pregnancy and after delivery if the baby is RhD positive¹².
Amniocentesis is a procedure where a needle is inserted into the uterus to obtain a sample of amniotic fluid, which contains fetal cells and other substances⁴. Amniocentesis can be done for various reasons, such as genetic testing, fetal lung maturity assessment, or infection diagnosis⁴. However, amniocentesis also carries a risk of causing bleeding or leakage of amniotic fluid, which can result in fetal-maternal hemorrhage (FMH), where fetal blood cells enter the maternal circulation⁴⁵. FMH can trigger RhD isoimmunization in RhD negative mothers, so they should receive RhIG within 72 hours of the procedure to prevent this complication⁵.
The other options are not correct because:
a) Hyperemesis gravidarum is not an indication for RhIG administration. Hyperemesis gravidarum is a condition where the mother experiences severe nausea and vomiting during pregnancy, which can cause dehydration, electrolyte imbalance, and weight loss. Hyperemesis gravidarum does not affect the blood type or compatibility of the mother and the baby, and does not increase the risk of RhD isoimmunization or HDN.
b) Rh-positive blood test results are not an indication for RhIG administration. Rh-positive blood test results mean that the mother has the RhD antigen on her red blood cells, and therefore she cannot develop antibodies against it¹². Rh-positive mothers do not need RhIG, as they are not at risk of RhD isoimmunization or HDN¹².
d) Anemia is not an indication for RhIG administration. Anemia is a condition where the mother has a low level of hemoglobin or red blood cells, which can cause fatigue, weakness, and shortness of breath. Anemia can have various causes, such as iron deficiency, bleeding, or infection. Anemia does not affect the blood type or compatibility of the mother and the baby, and does not increase the risk of RhD isoimmunization or HDN.
Correct Answer is C
Explanation
Ultrasonography is a diagnostic imaging technique that uses high-frequency sound waves to create images of the internal structures of the body. It is a safe and noninvasive method that can provide valuable information about the pregnancy, such as the number, size, location, and health of the fetus(es), the placenta, the amniotic fluid, and the uterus.
Ultrasonography can be performed at any time during pregnancy, but it is especially useful in the first trimester (the first 12 weeks of pregnancy) for several reasons, such as:
- To confirm the pregnancy and rule out ectopic pregnancy (a pregnancy that occurs outside the uterus) or molar pregnancy (a pregnancy that develops into an abnormal mass of tissue)
- To determine gestational age (the length of time since the first day of the last menstrual period) and estimate due date (the expected date of delivery)
- To screen for chromosomal abnormalities (such as Down syndrome) or structural defects (such as spina bifida) in the fetus
- To identify multiple gestations (such as twins or triplets) or complications (such as miscarriage or
bleeding)
One of the main uses of ultrasonography in the first trimester is to determine gestational age. This is important because it can affect many aspects of prenatal care and delivery, such as:
- The timing and accuracy of other tests and procedures
- The monitoring and evaluation of fetal growth and development
- The identification and management of potential problems or complications
- The planning and preparation for labor and delivery
Gestational age can be determined by measuring the crown-rump length (CRL) of the fetus, which is the distance from the top of the head to the bottom of the spine. The CRL can be measured by using a transvaginal ultrasound (an ultrasound probe that is inserted into the vagina) or a transabdominal ultrasound (an ultrasound probe that is moved over the abdomen). The CRL can be compared to a standard growth chart to estimate gestational age. The CRL measurement is most accurate between 7 and 13 weeks of pregnancy .
Therefore, the newly licensed nurse who says that ultrasound is used to determine gestational age in the first trimester indicates an understanding of the teaching.
The other statements show a lack of knowledge or misunderstanding of the uses of ultrasonography in the first trimester:
- a) "Ultrasound is used to observe for placental maturity in the first trimester." This is not correct because placental maturity is not assessed in the first trimester. Placental maturity refers to the changes that occur in the placenta as it ages and prepares for delivery. Placental maturity can be evaluated by using a grading system that ranges from 0 to 3, based on the appearance of calcifications (deposits of calcium) in the placenta. Placental maturity can be assessed by using a transabdominal ultrasound in the third trimester (after 28 weeks of pregnancy).
- b) "Ultrasound is used to detect intrauterine growth restriction in the first trimester." This is not correct because intrauterine growth restriction (IUGR) is not detected in the first trimester. IUGR is a condition in which the fetus does not grow as expected and has a low birth weight for its gestational age. IUGR can be caused by various factors, such as placental insufficiency, maternal malnutrition, infection, or chronic disease. IUGR can affect fetal development and increase the risk of complications, such as hypoxia, hypoglycemia, or stillbirth. IUGR can be diagnosed by measuring fetal growth parameters, such as abdominal circumference, head circumference, femur length, and estimated fetal weight. These measurements can be obtained by using a transabdominal ultrasound in the second or third trimester (after 20 weeks of pregnancy).
- d) "Ultrasound is used to perform a biophysical profile in the first trimester." This is not correct because a biophysical profile (BPP) is not performed in the first trimester. A BPP is a test that evaluates fetal well-being by assessing five parameters: fetal movement, fetal tone, fetal breathing, amniotic fluid volume, and fetal heart rate. A BPP can help detect fetal distress or hypoxia and guide management decisions. A BPP can be performed by using a combination of transabdominal ultrasound and nonstress test (NST) in the third trimester (after 32 weeks of pregnancy).
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today