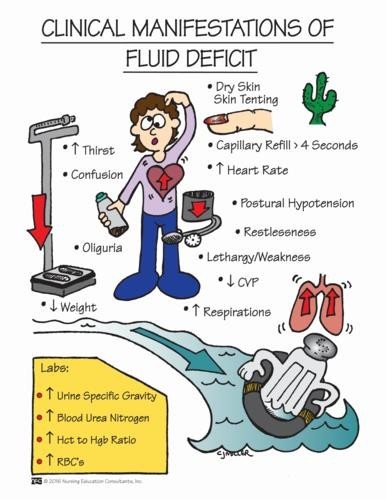
A nurse is caring for a client who is postoperative and is experiencing nausea and vomiting. The nurse should identify which of the following findings as indications that the client has fluid volume deficit. (Select all that apply.)
Full bounding pulse
Cool extremities
Moist crackles in the lungs
Orthostatic hypotension
Flat neck veins
Correct Answer : B,D,E
A: A full bounding pulse is a sign of increased fluid volume or fluid overload, not fluid volume deficit.
B: Cool extremities can be an indication of decreased peripheral perfusion, which may occur in fluid volume deficit.
C: Moist crackles in the lungs are an indication of fluid volume excess or pulmonary congestion, not fluid volume deficit.
D: Orthostatic hypotension, which is a drop in blood pressure when changing from lying to standing, can be a sign of fluid volume deficit due to inadequate blood volume.
E: Flat neck veins are an indication of decreased venous return and can occur in fluid volume deficit.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A: While explaining the negative consequences of refusal is important, it may not change the client's decision, and respect for the client's autonomy must be upheld.
B: Discussing the treatment with the client's partner without the client's consent may breach patient confidentiality and privacy.
C: Correct. The nurse should document the client's refusal of the medical treatment in the client's medical record. This documentation is essential for legal and ethical purposes and to ensure that the refusal is adequately communicated to the healthcare team.
D: Trying to convince the client to undergo the treatment is not appropriate and may violate the principle of informed consent. The client has the right to refuse treatment after being adequately informed of the risks and benefits.
Correct Answer is ["1820"]
Explanation
1. IV fluids:
- 150 mL/hr * 8 hr = 1200 mL
2. Juice:
- 4 oz * 30 mL/oz = 120 mL
3. Water:
- 0.5 L * 1000 mL/L = 500 mL
Total intake:
- 1200 mL + 120 mL + 500 mL = 1820 mL
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today