A nurse is caring for a client who is scheduled for surgery.
Exhibit 1
Medical History
0800:
Client has a history of malnutrition, hyperlipidemia, and diabetes mellitus.
Mini Nutritional Assessment screening tool score of 7 points (0 to 14 points)
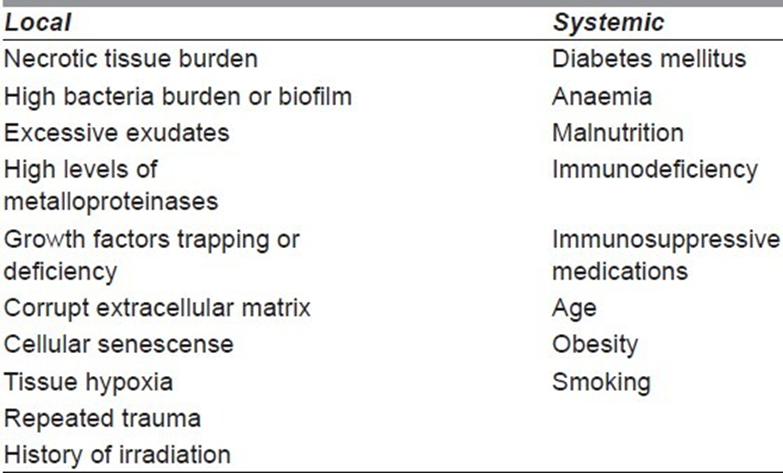
The nurse is reviewing the client's medical record. Which of the following findings places the client at risk for delayed wound healing? Select all that apply
History of diabetes mellitus
Cholesterol level
Prealbumin level
History of hyperlipidemia
Mini Nutritional Assessment screening tool score
History of malnutrition
Correct Answer : A,C,E,F
A. History of diabetes mellitus: This is correct. Diabetes mellitus can lead to delayed wound healing due to various factors, including impaired circulation, neuropathy, and compromised immune function.
B. Cholesterol level: While abnormal cholesterol levels can impact cardiovascular health, they are not directly linked to delayed wound healing unless they are part of a broader metabolic disorder or condition that affects vascular health.
C. Prealbumin level: Prealbumin is a marker of nutritional status. Low prealbumin levels can indicate malnutrition, which is a risk factor for delayed wound healing.
D. History of hyperlipidemia: Hyperlipidemia refers to high levels of fats (lipids) in the blood, such as cholesterol and triglycerides. While hyperlipidemia is associated with cardiovascular risk, it is not a direct risk factor for delayed wound healing unless it is part of a broader metabolic syndrome or condition affecting vascular health.
E. Mini Nutritional Assessment screening tool score: This is correct. The Mini Nutritional Assessment (MNA) screening tool assesses nutritional status, and a low score indicates malnutrition or nutritional deficiencies, which can contribute to delayed wound healing.
F. History of malnutrition: This is correct. Malnutrition, whether due to inadequate intake, absorption issues, or other factors, is a significant risk factor for delayed wound healing as it affects the body's ability to repair tissues and fight infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Uses one pair of gloves for dressing removal and irrigation:
It is essential to change gloves between different steps of wound care to prevent cross-contamination and infection. Using the same pair of gloves for dressing removal and irrigation increases the risk of introducing pathogens into the wound, which can lead to infection.
B. Uses a syringe with a catheter for wound irrigation.
Using a syringe with a catheter for wound irrigation allows for controlled and precise delivery of the irrigation solution to the wound site. It helps ensure that the wound is thoroughly cleansed without causing excessive pressure or trauma to the surrounding tissue.
C. Administers an analgesic medication 5 minutes before starting irrigation:
While administering analgesic medication may help alleviate the client's pain during wound irrigation, it is not directly related to the procedural aspect of wound irrigation. Pain management is an essential component of wound care, but it does not demonstrate an understanding of the specific procedure of wound irrigation.
D. Refrigerates the solution before irrigation:
Refrigerating the irrigation solution is not necessary and may cause discomfort to the client when cold solution is used for wound irrigation. Wound irrigation solutions are typically used at room temperature to avoid temperature-related discomfort and to maintain the integrity of the solution.
Correct Answer is D
Explanation
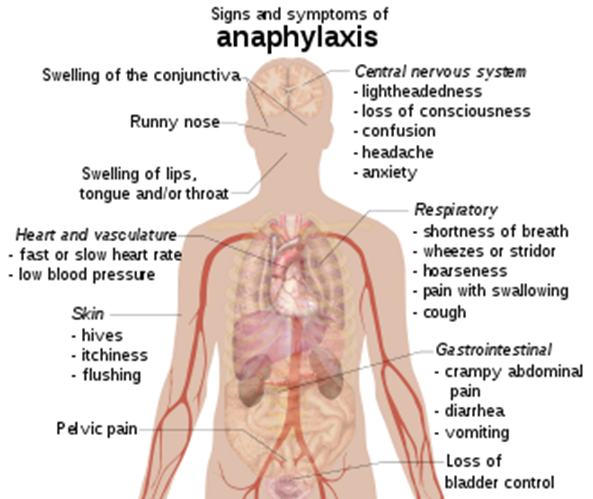
A. A feeling of swelling in the feet: Swelling in the feet can be caused by various factors such as fluid retention, circulatory issues, or certain medical conditions like venous insufficiency. It is not a typical symptom of anaphylaxis, which usually involves more generalized symptoms such as hives, itching, swelling of the face or throat, difficulty breathing, and a drop in blood pressure.
B. Pain at the injection site: Pain at the injection site is a common side effect of receiving an injection or medication. It occurs due to tissue irritation or trauma from the needle. While allergic reactions can cause localized redness, swelling, or itching at the injection site, severe pain alone is not a hallmark symptom of anaphylaxis.
C. A sudden decrease in heart rate: Anaphylaxis typically leads to an increase in heart rate (tachycardia) rather than a decrease. This increase in heart rate is a response to the body's attempt to compensate for the drop in blood pressure caused by anaphylaxis. Bradycardia (a decrease in heart rate) is not a typical feature of anaphylaxis unless it occurs very late in a severe reaction due to profound circulatory collapse.
D. A sharp decrease in blood pressure: This choice is indicative of an understanding of possible anaphylaxis. Anaphylaxis can cause a rapid and severe drop in blood pressure, known as hypotension. This drop in blood pressure is often a key feature of anaphylaxis and can lead to symptoms such as dizziness, fainting, confusion, and shock.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today