A nurse is checking a newborn’s Moro reflex.
Which of the following actions should the nurse take to elicit this reflex?
Place the newborn on their abdomen and observe the movement of their extremities.
Stroke the newborn’s cheek toward their mouth.
Stroke upward on the lateral aspect of the newborn’s foot.
Place the newborn on a flat surface and clap hands loudly.
The Correct Answer is D
Place the newborn on a flat surface and clap hands loudly.

This action will elicit the Moro reflex, also known as the startle reflex, which is a normal, involuntary reaction that newborns and infants have when they’re startled. In response to the sound, the baby will throw back his or her head, extend out his or her arms and legs, cry, then pull the arms and legs back in.
Choice A is wrong because placing the newborn on their abdomen and observing the movement of their extremities will not trigger the Moro reflex.
This position may elicit other reflexes such as the crawling reflex or the tonic neck reflex.
Choice B is wrong because stroking the newborn’s cheek toward their mouth will not trigger the Moro reflex. This action will elicit the rooting reflex, which helps the baby find the breast or bottle to start feeding.
Choice C is wrong because stroking upward on the lateral aspect of the newborn’s foot will not trigger the Moro reflex. This action will elicit the Babinski reflex, which causes the big toe to extend upward and the other toes to fan out.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Bleach.
According to the CDC, bleach is an effective disinfectant for environmental surfaces contaminated with blood or body fluids from a person with AIDS or other bloodborne pathogens. Bleach can kill HIV and hepatitis viruses when used in a 1:10 dilution with water.
Choice A is wrong because isopropyl alcohol is not recommended for disinfecting environmental surfaces. It can evaporate quickly and may not have enough contact time to kill the pathogens.
Choice B is wrong because chlorhexidine is an antiseptic, not a disinfectant. It is used for skin cleansing or wound irrigation, but it is not effective against spores or non-enveloped viruses.
Choice C is wrong because hydrogen peroxide is a low-level disinfectant that can be inactivated by organic matter.
It is not suitable for disinfecting surfaces contaminated with blood or body fluids.
Correct Answer is D
Explanation
Dysrhythmia is an abnormal heart rhythm that can be a sign of severe lithium toxicity.
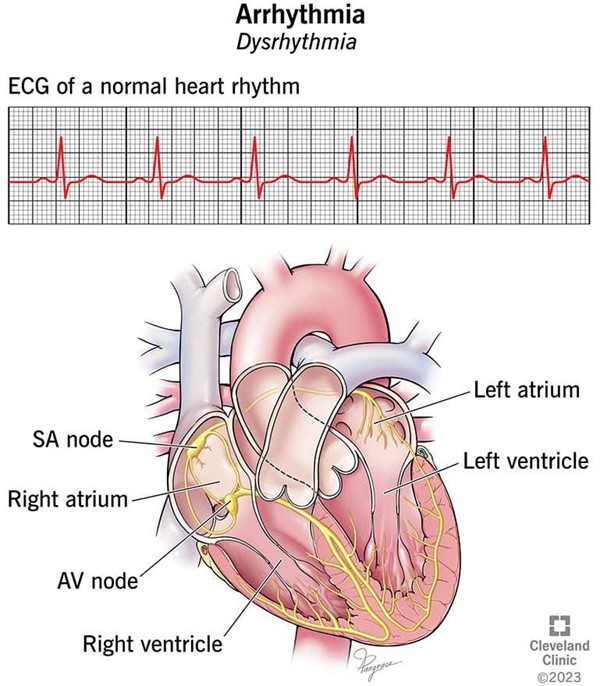
Lithium toxicity can occur when a person takes too much lithium, a mood- stabilizing medication used to treat bipolar disorder and major depressive disorder.
Choice A is wrong because hypoglycemia is not a symptom of lithium toxicity. Hypoglycemia is low blood sugar that can cause symptoms such as shakiness, sweating, hunger, and confusion.
Choice B is wrong because excess salivation is not a symptom of lithium toxicity. Excess salivation can be caused by various factors, such as infections, medications, or nerve damage.
Choice C is wrong because urinary retention is not a symptom of lithium toxicity. Urinary retention is the inability to empty the bladder completely, which can cause pain, discomfort, and infection. Lithium toxicity can actually cause increased urine output, not decreased.
Normal ranges for blood lithium levels are 0.6 to 1.2 mEq/L for maintenance therapy and 0.8 to 1.5 mEq/L for acute therapy. Levels above 1.5 mEq/L can cause mild to moderate toxicity, and levels above 2.0 mEq/L can cause severe toxicity. Levels above 3.0 mEq/L are considered a medical emergency.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today