A nurse is completing an assessment following suctioning of a child who has a tracheostomy. Which of the following findings should the nurse identify as an indication that the procedure has been effective?
Increased respiratory rate
Decreased oxygen saturation
Clear breath sounds
Increased oral secretions
The Correct Answer is C
A. Increased respiratory rate: An increased respiratory rate may indicate that the child is experiencing respiratory distress or discomfort, which could be a sign that suctioning was not effective or that it was too aggressive. Ideally, after suctioning, the child's respiratory rate should stabilize or decrease as they are able to breathe more comfortably with a clear airway.
B. Decreased oxygen saturation: A decreased oxygen saturation level may indicate that the child is not receiving enough oxygen, which could be a sign of ineffective suctioning or airway obstruction. Effective suctioning should improve oxygenation by removing secretions and allowing for better airflow. A decrease in oxygen saturation would suggest the need for further assessment and intervention.
C. Clear breath sounds: This is the correct option. Clear breath sounds indicate that the airway has been effectively cleared of excess secretions, allowing for clear airflow. After suctioning, the nurse should listen for clear breath sounds without any crackles, wheezes, or other abnormal sounds indicating obstruction or congestion.
D. Increased oral secretions: Increased oral secretions may suggest that suctioning was not effective in clearing secretions from the airway, leading to pooling of secretions in the mouth. Effective suctioning should remove excess secretions from the airway, reducing the need for excessive oral secretions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. FACES: The FACES pain scale is a visual analog scale commonly used with older children who can point to or select a facial expression that best represents their pain level. It may not be suitable for infants who may not have the cognitive or motor skills to use the scale effectively.
B. COMFORT: The COMFORT scale assesses pain in infants and young children based on behaviors such as crying, facial expressions, and body movements. It evaluates parameters such as alertness, calmness, respiratory response, physical movement, and muscle tone. The COMFORT scale is suitable for assessing pain in infants and young children, including those who are postoperative.
C. CRIES: The CRIES scale is a neonatal pain assessment tool that evaluates crying, oxygen saturation, vital signs, expression, and sleeplessness. While it is designed for newborns and infants up to 6 months of age, it may not be as appropriate for a 12-month-old infant who is postoperative and beyond the neonatal period.
D. FLACC: The FLACC scale assesses pain in infants and young children based on five behavioral categories: facial expression, leg movement, activity level, cry, and consolability. It is commonly used in pediatric settings and is suitable for assessing pain in infants who are postoperative.
Correct Answer is B
Explanation
A. Coarctation of the aorta
Coarctation of the aorta involves a narrowing of the aorta, leading to decreased blood flow to the lower body. It is not associated with increased pulmonary blood flow.
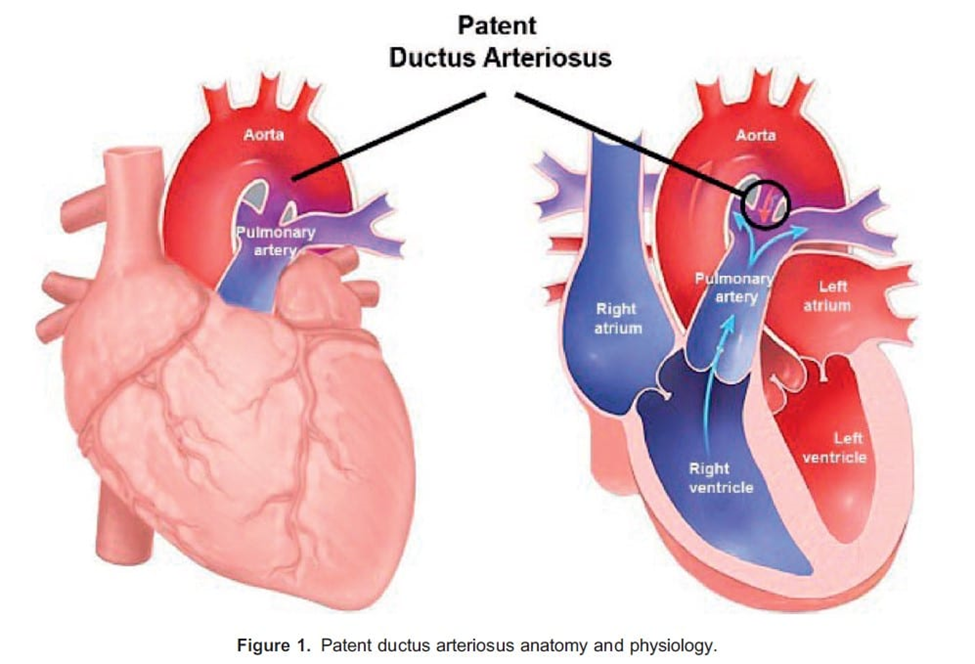
B. Patent ductus arteriosus
Patent ductus arteriosus (PDA) is a congenital heart defect where the ductus arteriosus, a fetal blood vessel that usually closes shortly after birth, remains open. This allows blood to flow from the aorta into the pulmonary artery, increasing pulmonary blood flow. Therefore, option B is correct.
C. Tetralogy of Fallot
Tetralogy of Fallot is a congenital heart defect characterized by four abnormalities, including a ventricular septal defect (VSD), pulmonary stenosis, right ventricular hypertrophy, and an overriding aorta. While it can lead to cyanosis due to right-to-left shunting, it is not primarily associated with increased pulmonary blood flow.
D. Tricuspid atresia
Tricuspid atresia involves the absence of the tricuspid valve, leading to a lack of direct blood flow from the right atrium to the right ventricle. It usually presents with decreased pulmonary blood flow rather than increased pulmonary blood flow.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today