A nurse provides education to a client recently diagnosed with macular degeneration. Which of the following statements made by the client requires reinforcement of education by the nurse?
"I will incorporate foods rich in vitamin C in my diet."
"I will receive injections into my eye."
"My vision will slowly be restored after I start using the eye drops."
"My vision will become progressively more blurry."
The Correct Answer is C
Choice A Reason: This is correct because incorporating foods rich in vitamin C in the diet can help prevent or delay macular degeneration. Vitamin C is an antioxidant that can protect the cells of the macula, which is the central part of the retina that is responsible for sharp and detailed vision, from oxidative stress and damage. The nurse should also advise the client to consume foods rich in other antioxidants, such as vitamin E, zinc, lutein, and zeaxanthin.
Choice B Reason: This is correct because receiving injections into the eye can help treat macular degeneration. Injections are a form of anti-vascular endothelial growth factor (anti-VEGF) therapy, which can block abnormal blood vessel growth and leakage in the macula that can cause vision loss. The nurse should explain to the client how often and how long they need to receive injections and what side effects or complications they may experience.
Choice C Reason: This is incorrect because vision will not be restored after using eye drops for macular degeneration. Eye drops are not a proven or effective treatment for macular degeneration, which is a chronic and progressive condition that causes irreversible vision loss. The nurse should reinforce education by informing the client that eye drops may only provide temporary relief of dryness or irritation, but they will not improve or restore vision.
Choice D Reason: This is correct because vision will become progressively more blurry with macular degeneration. Macular degeneration can cause blurred or distorted central vision, difficulty reading or recognizing faces, or dark spots in the visual field. The nurse should educate the client on how to cope with vision loss and use adaptive devices, such as magnifiers, large-print books, or voice-activated technology.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
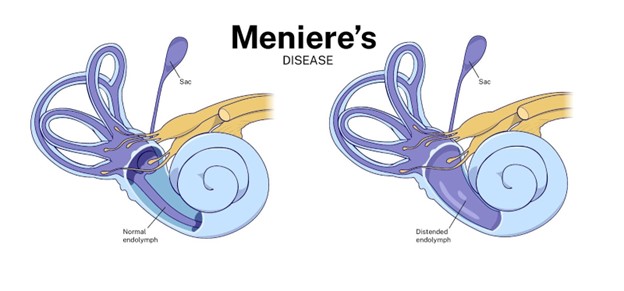
Choice A Reason: This is incorrect because Ménière's disease is not caused by an allergic response. Ménière's disease is a disorder of the inner ear that causes vertigo, tinnitus, hearing loss, and a feeling of fullness in the ear. The exact cause of Ménière's disease is unknown, but it may be related to fluid imbalance, infection, trauma, or autoimmune reaction.
Choice B Reason: This is correct because diphenhydramine can help offset the nauseous feeling. Diphenhydramine is an antihistamine that blocks histamine receptors in the brain and inner ear, which can reduce nausea and vomiting associated with vertigo.
Choice C Reason: This is correct because anticholinergics will help you rest. Anticholinergics are a class of drugs that block acetylcholine receptors in the brain and body, which can have sedative effects and reduce motion sickness. Diphenhydramine has anticholinergic properties.
Choice D Reason: This is correct because diphenhydramine can help reduce vomiting episodes. As mentioned above, diphenhydramine can reduce nausea and vomiting by blocking histamine receptors in the brain and inner ear.
Correct Answer is A
Explanation
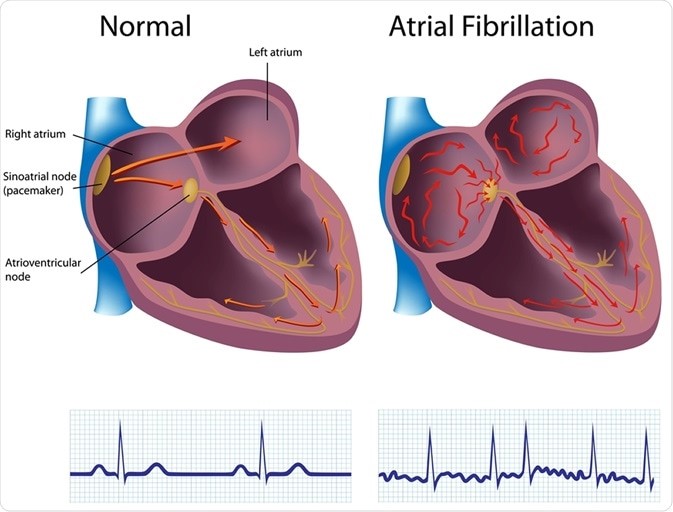
Choice A reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at
the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
Choice B reason: This is incorrect because hypertension is not the risk factor that puts the client at
the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
Choice C reason: This is incorrect because diabetes is not the risk factor that puts the client at
the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
Choice D reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at
the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today