A woman is in active labor. On spontaneous rupture of her membranes, the nurse caring for this woman notices variable deceleration patterns during evaluation of the monitor tracing. When preparing to perform a vaginal examination, the nurse observes a small section of the umbilical cord protruding from the vagina. What should the nurse do next?
Wrap the cord loosely with a sterile towel saturated with warm normal saline.
Place a sterile gloved hand into the vagina and hold the presenting part off the cord while calling for assistance.
Increase the IV drip rate.
Administer oxygen to the woman via mask at 8 to 10 L/minute.
The Correct Answer is B
Choice A) Wrap the cord loosely with a sterile towel saturated with warm normal saline: This is not an appropriate action because it does not relieve the compression of the cord, which can cause fetal hypoxia and acidosis. The cord should be kept moist, but not wrapped around anything.
Choice B) Place a sterile gloved hand into the vagina and hold the presenting part off the cord while calling for assistance: This is the correct action because it prevents further descent of the fetus and reduces the pressure on the cord, which can improve fetal oxygenation and blood flow. The nurse should also elevate the woman's hips and place her in a knee-chest or Trendelenburg position to reduce gravity. The nurse should call for immediate assistance and prepare for an emergency cesarean section.
Choice C) Increase the IV drip rate: This is not an appropriate action because it does not address the cause of the variable decelerations, which is cord compression. Increasing the IV fluid may cause fluid overload and worsen maternal and fetal outcomes.
Choice D) Administer oxygen to the woman via mask at 8 to 10 L/minute: This is not an appropriate action because it does not relieve the cord compression, which is the main threat to fetal well-being. Oxygen administration may be helpful in some cases of fetal distress, but it is not sufficient in this situation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A) Monitor uterine contractions is incorrect because this is not the most urgent intervention for a pregnant woman who has experienced a bleeding episode in late pregnancy. Uterine contractions can indicate labor or placental abruption, which are possible causes of bleeding in late pregnancy. However, they are not the only or the most reliable indicators of these conditions, as some women may have painless bleeding or contractions without bleeding. Moreover, monitoring uterine contractions does not address the immediate needs of the mother and the fetus, such as oxygenation, circulation, and perfusion. Therefore, this intervention should be done after assessing and stabilizing the vital signs and FHR.
Choice B) Assess fetal heart rate (FHR) and maternal vital signs is correct because this is the most important and essential intervention for a pregnant woman who has experienced a bleeding episode in late pregnancy. Bleeding in late pregnancy can be caused by various conditions, such as placenta previa, placental abruption, uterine rupture, or vasa previa, which can compromise the blood supply and oxygen delivery to the mother and the fetus. Assessing FHR and maternal vital signs can help to determine the severity and cause of the bleeding, as well as guide further
interventions such as fluid resuscitation, oxygen therapy, blood transfusion, or emergency delivery. The normal FHR range for a fetus is 110 to 160 beats per minute, and it may vary with fetal activity or maternal position. The normal maternal vital signs are: blood pressure 120/80 mm Hg or lower, heart rate 60 to 100 beats per minute, respiratory rate 12 to 20 breaths per minute, and temperature 36.5°C to 37.5°C (97.7°F to 99.5°F). Any deviation from these ranges may indicate hypoxia, hypovolemia, shock, infection, or distress. Therefore, this intervention should be done as soon as possible for women who have bleeding in late pregnancy.
Choice c) Perform a venipuncture for hemoglobin and hematocrit levels is incorrect because this is not a priority intervention for a pregnant woman who has experienced a bleeding episode in late pregnancy. Hemoglobin and hematocrit are blood tests that measure the amount of red blood cells and their percentage in the blood volume.
They can help to evaluate the extent of blood loss and the need for blood transfusion. However, they are not
immediate or accurate indicators of bleeding in late pregnancy, as they may take time to reflect the changes in blood volume or be affected by other factors such as hydration or hemodilution. Moreover, performing a venipuncture does not address the immediate needs of the mother and the fetus, such as oxygenation, circulation, and perfusion.
Therefore, this intervention should be done after assessing and stabilizing the vital signs and FHR.
Choice d) Place clean disposable pads to collect any drainage is incorrect because this is not a priority intervention for a pregnant woman who has experienced a bleeding episode in late pregnancy. Placing clean disposable pads can help to keep the perineal area clean and dry, as well as to estimate the amount and type of bleeding. However, it does not address the immediate needs of the mother and the fetus, such as oxygenation, circulation, and perfusion. Moreover, it does not provide any information about the cause or severity of the bleeding, as it may be affected by factors such as gravity or pooling. Therefore, this intervention should be done after assessing and stabilizing the vital signs and FHR.
Correct Answer is A
Explanation
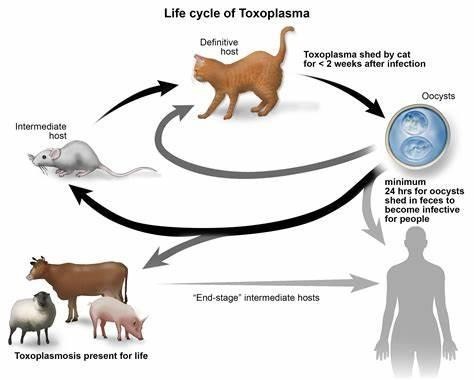
Choice a) I will be certain to empty the litter boxes regularly is incorrect because this is a risky behavior for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis is an infection caused by a parasite called Toxoplasma gondii, which can be found in the feces of cats and other animals. If a pregnant woman gets infected with toxoplasmosis, she can pass it to her unborn baby, which can cause serious problems such as miscarriage, stillbirth, or birth defects. Therefore, a pregnant woman should avoid contact with cat litter and let someone else handle the litter boxes, or wear gloves and wash her hands thoroughly if she has to do it herself.
Choice b) I have to wash all of my fruits and vegetables is correct because this is a good practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be transmitted through contaminated soil or water, which can adhere to fruits and vegetables. Therefore, a pregnant woman should wash all of her fruits and vegetables before eating them, and peel or cook them if possible, to remove any traces of the parasite.
Choice c) I won't eat raw eggs is correct because this is another good practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be acquired through eating undercooked or raw meat or eggs that contain the parasite. Therefore, a pregnant woman should avoid eating raw eggs or any foods that contain them, such as mayonnaise, mousse, or homemade ice cream, and cook all of her meat and eggs thoroughly until they are no longer pink or runny.
Choice d) I need to be cautious when cooking meat is correct because this is also an important practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be spread through handling raw meat that contains the parasite. Therefore, a pregnant woman should be careful when cooking meat and use separate utensils and cutting boards for raw and cooked meat, wash her hands and surfaces after touching raw meat, and avoid tasting raw meat while cooking it.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today