A nurse is monitoring a patient who is receiving a blood transfusion.
Which of the following symptoms should the nurse report to the charge nurse as a sign of an allergic blood transfusion reaction?
Bilateral flank pain.
Distended jugular veins.
Generalized urticaria.
Blood pressure 184/92 mm Hg.
The Correct Answer is C
Choice A rationale:
Bilateral flank pain is not a typical sign of an allergic blood transfusion reaction. It can be associated with other conditions, such as kidney problems, musculoskeletal issues, or abdominal aortic aneurysm. While it's important to assess flank pain, it doesn't directly suggest an allergic reaction to the transfusion.
Choice B Rationale:
Distended jugular veins can indicate fluid overload, which could potentially occur during a transfusion. However, it's not a specific sign of an allergic reaction. Fluid overload can result from various causes, including heart failure, kidney problems, or excessive fluid intake. It's crucial to monitor for fluid overload during transfusions, but it doesn't definitively point to an allergic reaction.
Choice C Rationale:
Generalized urticaria, or hives, is a hallmark sign of an allergic reaction. It's characterized by raised, red, itchy welts that can appear on various parts of the body. Hives can develop rapidly and spread extensively. During a blood transfusion, generalized urticaria strongly suggests that the patient's immune system is reacting to a component of the transfused blood, such as proteins or antibodies.

Choice D Rationale:
Blood pressure 184/92 mm Hg is elevated and could be concerning, but it's not specific to allergic reactions. High blood pressure can have various causes, including stress, pain, anxiety, or underlying hypertension. While monitoring blood pressure during transfusions is essential, it doesn't directly indicate an allergic reaction.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale:
The spinal cord plays a crucial role in pain transmission, but it does not initiate the afferent pathways. It receives pain signals from nociceptors and relays them to the brain for processing.
The spinal cord is also involved in pain modulation, as it can dampen or amplify pain signals depending on various factors. However, it is not the primary trigger for pain sensation. That role belongs to nociceptors.
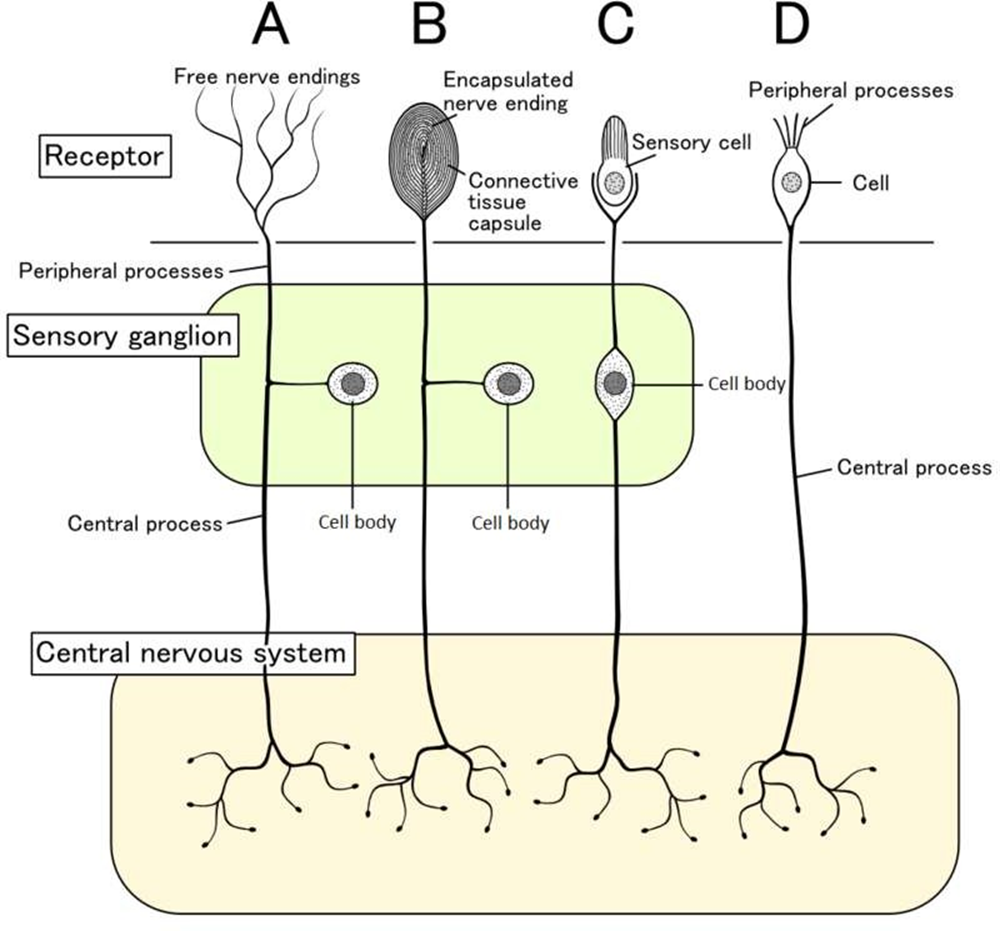
Choice B rationale:
Nociceptors are specialized sensory receptors that detect potentially damaging stimuli, such as intense heat, pressure, or chemical irritants.
They are located throughout the body, including the skin, muscles, joints, and internal organs.
When nociceptors are activated, they generate electrical signals that travel along nerve fibers to the spinal cord and brain. This process initiates the afferent pathways, which ultimately lead to the conscious perception of pain.
Nociceptors are essential for protecting the body from harm. They alert us to potential dangers and trigger responses that help us avoid injury or further damage.
Choice C rationale:
Endorphins are natural pain-relieving substances produced by the body. They act on receptors in the brain and spinal cord to reduce pain perception.
However, endorphins do not trigger the afferent pathways. They work by modulating pain signals that have already been initiated by nociceptors.
Choice D rationale:
The cortex is the outer layer of the brain that is responsible for higher-level functions, such as thinking, feeling, and decision- making.
It plays a role in the conscious experience of pain, but it does not trigger the afferent pathways.
The cortex receives pain signals from the spinal cord and processes them, leading to the awareness of pain.
Correct Answer is D
Explanation
Choice A rationale:
Serosanguineous drainage is a mixture of blood serum and blood. It is typically thin and watery, with a pinkish or reddish hue.
It is common in the early stages of wound healing, as small blood vessels are injured and release their contents. However, it's not consistent with the yellow and thick drainage described in the question, making it an unlikely choice.
Choice B Rationale:
Serous drainage is clear and watery, composed primarily of blood plasma.
It's also common in the early stages of wound healing and is considered a normal part of the process. However, the clear and watery nature of serous drainage doesn't match the thick, yellow drainage described in the question, ruling out this option.
Choice C Rationale:
Sanguineous drainage is composed primarily of fresh blood.
It's often bright red and may be thick or thin, depending on the amount of bleeding. While sanguineous drainage can indicate a problem, it's typically associated with active bleeding or recent trauma. The yellow color of the drainage in the question makes this choice less likely.
Choice D Rationale:
Purulent drainage is a thick, yellow, green, or brown fluid that often has a foul odor.
It's a sign of infection, as it contains dead white blood cells, bacteria, and debris. The yellow and thick consistency of the drainage described in the question strongly suggests purulent drainage, making it the most likely answer.
Key Points:
The color, consistency, and odor of wound drainage can provide valuable clues about the healing process and potential complications.
Purulent drainage is a hallmark of infection and requires prompt attention.
Nurses play a crucial role in assessing wound drainage and reporting any concerns to the healthcare team.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today