When assessing a multigravida on the first postpartum day, the nurse finds a moderate amount of lochia rubra, with the uterus firm and three fingerbreadths above the umbilicus. What action should the nurse implement first?
Check for a distended bladder.
Review the hemoglobin to determine hemorrhage.
Massage the uterus to decrease atony.
Increase intravenous infusion.
The Correct Answer is A
Choice A reason: This is the correct answer because a distended bladder can cause uterine displacement and interfere with uterine contraction, leading to increased bleeding and risk of infection. The nurse should check for bladder fullness and encourage the client to void or catheterize if necessary.
Choice B reason: Reviewing the hemoglobin to determine hemorrhage is an important action, but not the first one. The nurse should first identify and correct the cause of bleeding, such as bladder distension or uterine atony, before checking for blood loss and anemia.
Choice C reason: Massaging the uterus to decrease atony is not indicated in this case, because the uterus is already firm. Massaging a firm uterus can cause overstimulation and pain.
Choice D reason: Increasing intravenous infusion is not the first action, because it may worsen bleeding by increasing blood pressure and diluting clotting factors. The nurse should first assess and manage bleeding before administering fluids or blood products as prescribed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Administering a half dose now is not advisable, because it may result in underdosing or overdosing of digoxin. Digoxin has a narrow therapeutic range and a high risk of toxicity, especially in infants and children. The amount of digoxin absorbed by the infant before vomiting is unknown, so giving a partial dose may not achieve therapeutic levels or may exceed safe levels.
Choice B reason: Giving another dose is not advisable, because it may result in overdosing of digoxin. Digoxin has a narrow therapeutic range and a high risk of toxicity, especially in infants and children. The amount of digoxin absorbed by the infant before vomiting is unknown, so giving a full dose may exceed safe levels and cause adverse effects such as nausea, vomiting, bradycardia, arrhythmias, or visual disturbances.
Choice C reason: Mixing the next dose with food is not advisable, because it may affect the absorption and bioavailability of digoxin. Digoxin should be taken on an empty stomach or at least one hour before or two hours after meals, because food can interfere with its absorption from the gastrointestinal tract and reduce its effectiveness.
Choice D reason: Withholding this dose is the best instruction for the nurse to provide to this mother. Digoxin has a long half-life and accumulates in tissues, so missing one dose will not significantly affect its therapeutic effect. Withholding this dose will avoid overdosing and toxicity of digoxin, which can be life-threatening in infants and children. The nurse should also advise the mother to resume the regular dosing schedule and monitor the infant's pulse rate and signs of digoxin toxicity.
Correct Answer is A
Explanation
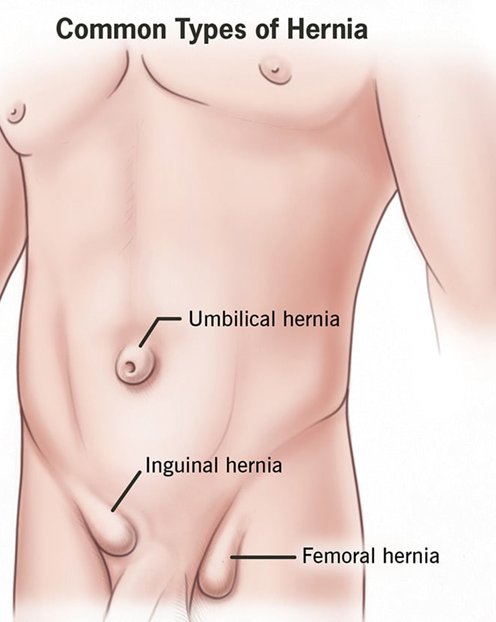
Choice A reason: This hernia is a normal variation that resolves without treatment is a correct explanation for the nurse to provide, as this refers to an umbilical hernia, which is a common and harmless condition in infants that usually disappears by age 2. Therefore, this is the correct choice.
Choice B reason: An abdominal binder can be worn daily to reduce the protrusion is not an appropriate explanation for the nurse to provide, as this is not an effective or recommended method to treat a hernia. This is a distractor choice.
Choice C reason: Restrictive clothing will be adequate to help the hernia go away is not a relevant explanation for the nurse to provide, as this does not affect the hernia or its resolution. This is another distractor choice.
Choice D reason: The quarter should be secured with an elastic bandage wrap is not a sensible explanation for the nurse to provide, as this is a folk remedy that has no scientific basis and can cause skin irritation and infection. This is another distractor choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today