The nurse administers amiodarone to a client with ventricular tachycardia. Which monitoring by the nurse is necessary with this drug? (Select all that apply)
QT interval
Heart rate
Respiratory rate
Heart rhythm
Urine output
Correct Answer : A,B,C,D,E
Choice A Reason:
Monitoring the QT interval is crucial when administering amiodarone because this drug can prolong the QT interval, increasing the risk of torsades de pointes, a potentially life-threatening type of ventricular tachycardia. Regular monitoring helps in early detection and management of this adverse effect, ensuring patient safety.
Title: Choice B Reason:
Heart rate monitoring is essential as amiodarone can cause bradycardia (slow heart rate). Continuous monitoring allows the nurse to detect any significant changes in heart rate and take appropriate actions, such as adjusting the medication dosage or providing interventions to manage bradycardia.
Title: Choice C Reason:
Respiratory rate monitoring is necessary because amiodarone can cause pulmonary toxicity, including interstitial pneumonitis and acute respiratory distress syndrome (ARDS). By keeping track of the respiratory rate, the nurse can identify early signs of respiratory complications and intervene promptly
Title: Choice D Reason:
Heart rhythm monitoring is vital since amiodarone is used to treat arrhythmias. Continuous electrocardiogram (ECG) monitoring helps in assessing the effectiveness of the drug in controlling arrhythmias and detecting any new or worsening arrhythmias that may require immediate attention.
Title: Choice E Reason:
Monitoring urine output is important because amiodarone can affect renal function, especially in patients with pre-existing kidney conditions. Keeping track of urine output helps in assessing renal function and ensuring that the drug is not causing nephrotoxicity
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: You May Bring Some Music to Listen to for Distraction
Bringing music for distraction is generally not a standard instruction given before an EEG. While listening to music might help some patients relax, it is not a critical part of the preparation for the test. The primary focus of EEG preparation is to ensure accurate readings of brain activity, which can be influenced by various factors such as medication and sleep.
Choice B: Do Not Take Any Sedatives 12 to 24 Hours Before the Test
Avoiding sedatives before an EEG is crucial because these medications can alter brain activity and affect the test results. Sedatives can suppress the electrical activity in the brain, leading to inaccurate readings. Therefore, it is essential for patients to avoid taking any sedatives 12 to 24 hours before the test to ensure the EEG captures the brain’s natural activity.
Choice C: You Will Need to Have Someone to Drive You Home
This instruction is typically given if the patient is expected to be sedated or if the test involves procedures that might impair their ability to drive. However, for a standard EEG, patients are usually not sedated, and there is no need for someone to drive them home. This instruction is more relevant for other types of medical procedures that involve sedation.
Choice D: Please Do Not Have Anything to Eat or Drink After Midnight
Fasting is not a standard requirement for an EEG. Patients are generally allowed to eat and drink before the test. However, they are often advised to avoid caffeine as it can affect brain activity. The instruction to avoid food and drink after midnight is more commonly associated with procedures that require anesthesia or sedation, not an EEG.
Correct Answer is B
Explanation
Choice A Reason:
Decrease protein intake: This is not typically recommended for clients with Cushing’s disease. Protein is essential for maintaining muscle mass and overall health. Clients with Cushing’s disease often experience muscle weakness and wasting, so adequate protein intake is crucial to help counteract these effects. Therefore, decreasing protein intake would not be beneficial.
Choice B Reason:
Restrict sodium intake: Clients with Cushing’s disease often suffer from hypertension (high blood pressure) due to the excess cortisol in their bodies. High sodium intake can exacerbate this condition by increasing blood pressure even further. Therefore, it is crucial to restrict sodium intake to help manage hypertension and reduce the risk of cardiovascular complications. Foods high in sodium include processed foods, canned soups, and salty snacks. The recommended daily sodium intake for most adults is less than 2,300 milligrams, but for those with hypertension, it is often advised to consume even less.
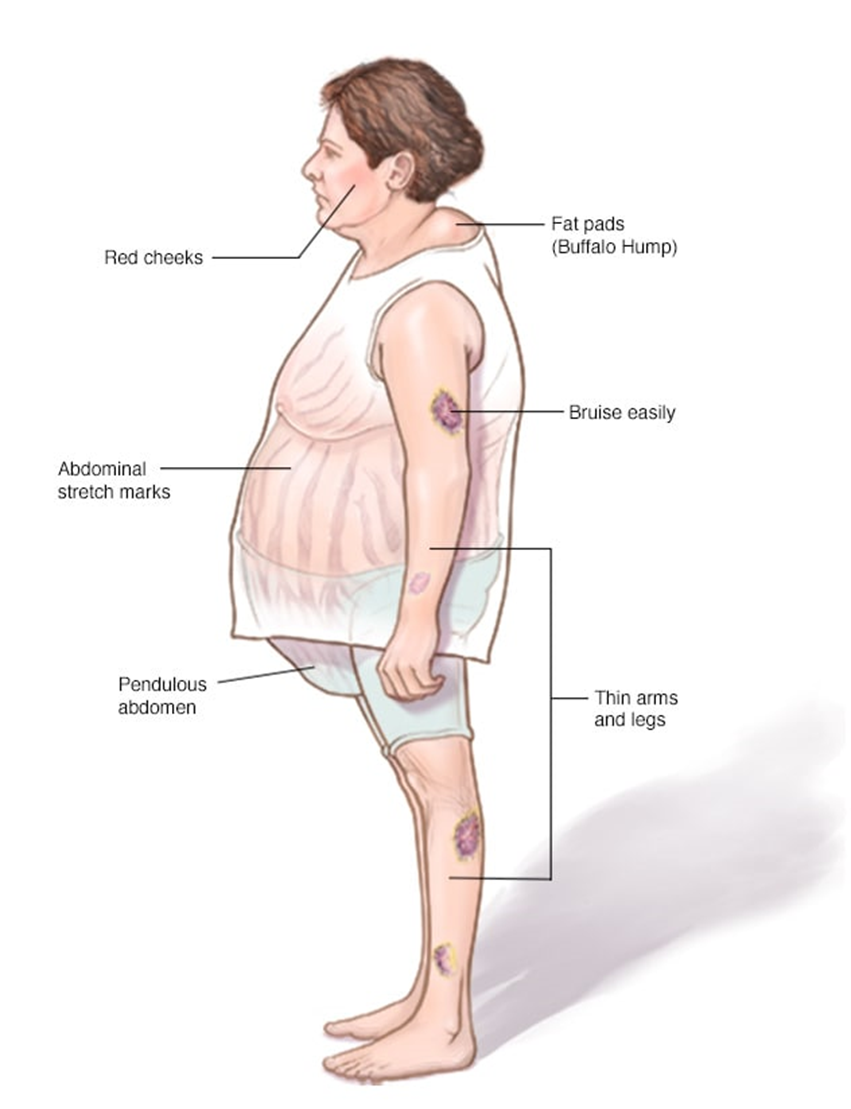
Choice C Reason:
Limit intake of potassium-rich foods: This is not a standard recommendation for clients with Cushing’s disease. In fact, potassium is often beneficial as it can help counteract the effects of sodium and lower blood pressure. Potassium-rich foods include bananas, oranges, spinach, and sweet potatoes. Limiting these foods would not be advantageous and could potentially worsen hypertension.
Choice D Reason:
Increase carbohydrate intake: Increasing carbohydrate intake is not typically recommended for clients with Cushing’s disease. Excess cortisol can lead to increased blood sugar levels and a higher risk of developing diabetes. Therefore, it is important to manage carbohydrate intake carefully to avoid spikes in blood sugar. Instead, a balanced diet with a focus on complex carbohydrates, lean proteins, and healthy fats is recommended.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today