The nurse is caring for a child with acute renal failure. Which clinical manifestation should the nurse recognize as a sign of hyperkalemia?
Cardiac arrhythmia
Seizure
Dyspnea
Oliguria
The Correct Answer is A
Choice A reason:
Cardiac arrhythmia is a primary clinical manifestation of hyperkalemia. Hyperkalemia, defined as an elevated level of potassium in the blood, can significantly affect the electrical activity of the heart. This can lead to various types of arrhythmias, including bradycardia, ventricular tachycardia, and even cardiac arrest1. The presence of arrhythmias is a critical indicator of hyperkalemia and requires immediate medical attention to prevent life-threatening complications.
Choice B reason:
Seizures are not typically associated with hyperkalemia2. While severe electrolyte imbalances can potentially lead to neurological symptoms, seizures are more commonly linked to conditions such as hyponatremia (low sodium levels) or hypocalcemia (low calcium levels). Therefore, seizures are not a primary sign of hyperkalemia.
Choice C reason:
Dyspnea, or difficulty breathing, can occur in various medical conditions, including heart failure and respiratory disorders. While hyperkalemia can lead to muscle weakness and fatigue, which might indirectly affect breathing, dyspnea is not a primary clinical manifestation of hyperkalemia. The main concern with hyperkalemia is its effect on cardiac function.
Choice D reason:
Oliguria, or reduced urine output, is a symptom of acute renal failure but not specifically indicative of hyperkalemia. While acute renal failure can lead to hyperkalemia due to the kidneys’ inability to excrete potassium, oliguria itself is not a direct sign of hyperkalemia. The focus should be on the cardiac effects of elevated potassium levels
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","C"]
Explanation
The correct answers are a) Use a straw to administer the medication, b) Give the medication with vitamin C, and c) It is best to give the medication with food.
Choice A reason:
Using a straw to administer ferrous sulfate is recommended to prevent staining of the teeth. Ferrous sulfate, especially in liquid form, can cause discoloration of the teeth if it comes into direct contact with them. By using a straw, the medication bypasses the teeth, reducing the risk of staining.
Choice B reason:
Giving ferrous sulfate with vitamin C is beneficial because vitamin C enhances the absorption of iron. Vitamin C (ascorbic acid) helps convert iron into a form that is more easily absorbed by the body. Therefore, administering ferrous sulfate with a source of vitamin C, such as orange juice, can improve its effectiveness.
Choice C reason:
It is best to give ferrous sulfate with food to reduce gastrointestinal side effects. While iron is best absorbed on an empty stomach, it can cause stomach upset, nausea, and constipation. Taking the medication with food can help mitigate these side effects, making it more tolerable for the child.
Choice D reason:
Giving ferrous sulfate with milk is not recommended. Dairy products, including milk, can interfere with the absorption of iron. Calcium in milk binds with iron, reducing its bioavailability and effectiveness. Therefore, it is best to avoid giving ferrous sulfate with milk or other dairy products.
Correct Answer is D
Explanation
Choice A reason:
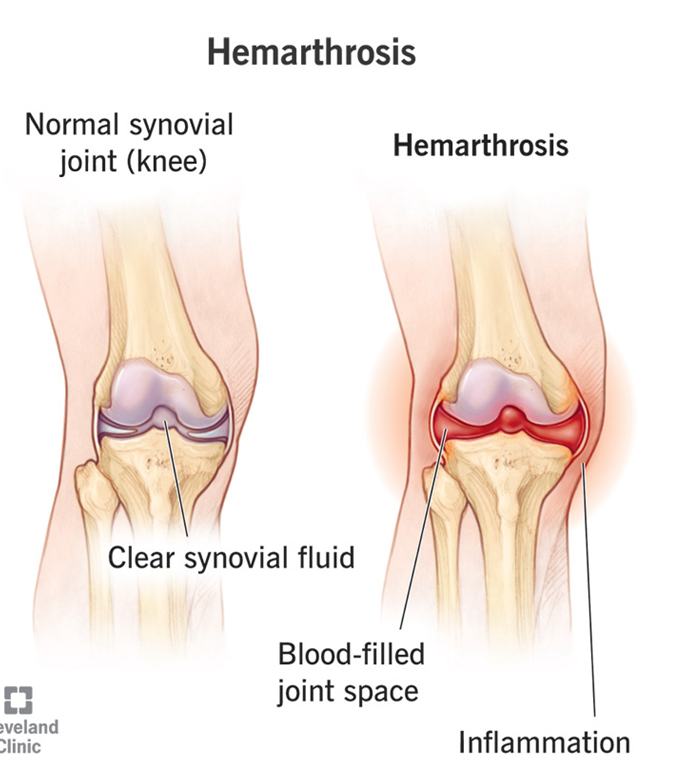
Keeping the affected extremity below the level of the heart is not recommended in the management of hemarthrosis in a child with hemophilia A. Elevating the affected limb can help reduce swelling and pain by promoting venous return and decreasing pressure in the joint.
Choice B Reason:
The use of topical analgesic cream on the painful area is not a primary treatment for hemarthrosis in hemophilia A. While it may provide some temporary relief, it does not address the underlying issue of bleeding within the joint. The primary treatment involves replacing the missing clotting factor.
Choice C Reason:
Instructing the parent to call their health care provider to obtain a plan of care is important, but it is not the immediate management step for hemarthrosis. Prompt treatment with clotting factor replacement is crucial to stop the bleeding and prevent joint damage.
Choice D Reason:
Prompt infusion of Factor VIII is the primary treatment for hemarthrosis in a child with hemophilia A. This treatment helps to replace the missing clotting factor, stop the bleeding, and prevent further joint damage. Early intervention is essential to minimize complications and promote healing.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today