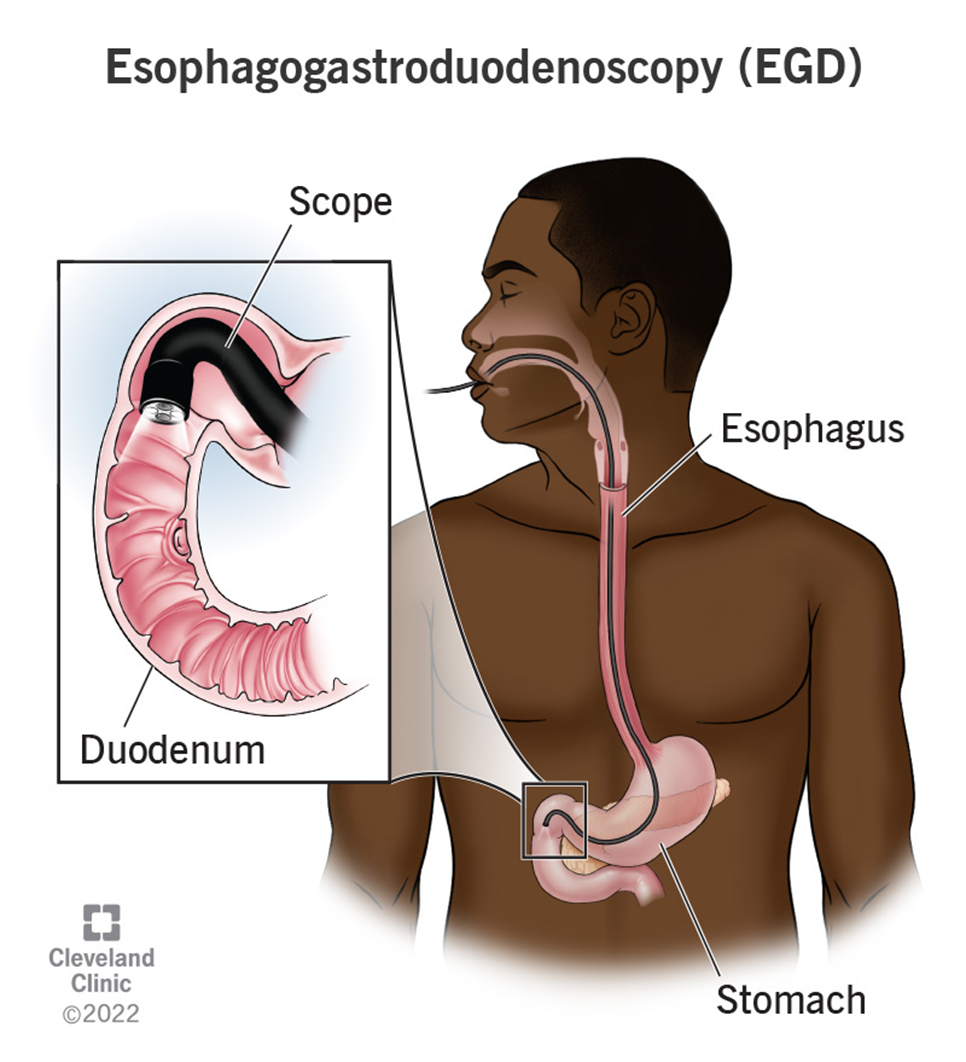
The nurse is caring for a client recovering from an esophagogastroduodenoscopy (EGD). Which of the following client symptoms would require further nursing assessment?
Thirst
Sore throat
Abdominal distention
Drowsiness
The Correct Answer is C
Choice A Reason:
Thirst is a common and expected symptom after an EGD, especially if the client has been fasting before the procedure. It does not typically indicate a complication and can be managed by gradually reintroducing fluids as tolerated. Therefore, thirst does not require further nursing assessment beyond routine post-procedure care.
Choice B Reason:
A sore throat is also a common symptom following an EGD. The procedure involves passing an endoscope through the throat, which can cause temporary irritation and discomfort. This symptom usually resolves on its own within a few days and does not indicate a serious complication. Therefore, a sore throat does not require further nursing assessment beyond providing comfort measures such as lozenges or warm saltwater gargles.
Choice C Reason:
Abdominal distention is a concerning symptom that requires further nursing assessment. It can indicate complications such as perforation, bleeding, or infection following the EGD. Perforation of the gastrointestinal tract is a rare but serious complication that can lead to peritonitis and sepsis if not promptly addressed. Therefore, any signs of abdominal distention should be reported to the provider immediately for further evaluation and intervention.
Choice D Reason:
Drowsiness is a common side effect of the sedatives used during the EGD procedure. It is expected that the client may feel drowsy or sleepy for a few hours after the procedure as the sedative wears off. This symptom does not typically require further nursing assessment unless it persists for an unusually long time or is accompanied by other concerning symptoms such as difficulty breathing or altered mental status.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: You May Bring Some Music to Listen to for Distraction
Bringing music for distraction is generally not a standard instruction given before an EEG. While listening to music might help some patients relax, it is not a critical part of the preparation for the test. The primary focus of EEG preparation is to ensure accurate readings of brain activity, which can be influenced by various factors such as medication and sleep.
Choice B: Do Not Take Any Sedatives 12 to 24 Hours Before the Test
Avoiding sedatives before an EEG is crucial because these medications can alter brain activity and affect the test results. Sedatives can suppress the electrical activity in the brain, leading to inaccurate readings. Therefore, it is essential for patients to avoid taking any sedatives 12 to 24 hours before the test to ensure the EEG captures the brain’s natural activity.
Choice C: You Will Need to Have Someone to Drive You Home
This instruction is typically given if the patient is expected to be sedated or if the test involves procedures that might impair their ability to drive. However, for a standard EEG, patients are usually not sedated, and there is no need for someone to drive them home. This instruction is more relevant for other types of medical procedures that involve sedation.
Choice D: Please Do Not Have Anything to Eat or Drink After Midnight
Fasting is not a standard requirement for an EEG. Patients are generally allowed to eat and drink before the test. However, they are often advised to avoid caffeine as it can affect brain activity. The instruction to avoid food and drink after midnight is more commonly associated with procedures that require anesthesia or sedation, not an EEG.
Correct Answer is ["C","E"]
Explanation
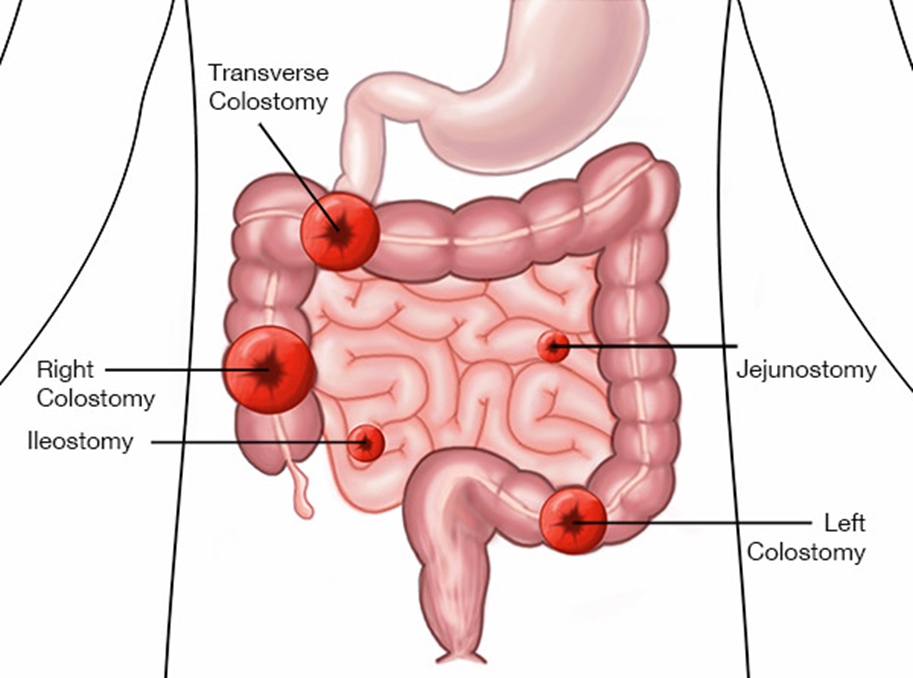
Choice A: Formed stool in collection pouch
Formed stool in the collection pouch is not expected in an ileostomy. The output from an ileostomy is typically liquid to semi-liquid because the ileum does not absorb as much water as the colon. If formed stool is present, it may indicate a blockage or other issue that needs to be addressed.
Choice B: Stoma is edematous and bleeding
An edematous and bleeding stoma is not a normal finding and may indicate complications such as infection, trauma, or poor stoma care. The stoma should be moist and pink, but not swollen or bleeding. Persistent bleeding or significant edema should be reported to a healthcare provider immediately.
Choice C: Stoma is pink and shiny
A pink and shiny stoma is a sign that the ileostomy is functioning well. This indicates good blood flow and healthy tissue. The stoma should always appear moist and pink, similar to the inside of the mouth. Any deviation from this appearance, such as a pale, dark, or dry stoma, should be evaluated by a healthcare professional.
Choice D: Skin excoriation around the stoma
Skin excoriation around the stoma is not a normal finding and suggests that the skin is being irritated by the stoma output or the ostomy appliance. Proper skin care and fitting of the ostomy appliance are essential to prevent skin breakdown. If excoriation occurs, it should be treated promptly to prevent further complications.
Choice E: Mucus liquid flows from the stoma
Mucus liquid flowing from the stoma is expected in an ileostomy. The output is typically liquid to semi-liquid and may contain mucus, which is normal for the small intestine. This type of output indicates that the ileostomy is functioning as intended.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today