PPH may be sudden and result in rapid blood loss.
The nurse must be alert to the symptoms of hemorrhage and hypovolemic shock and be prepared to act quickly to minimize blood loss.
Astute assessment of circulatory status can be done with noninvasive monitoring.
Please match the type of noninvasive assessment that the RN would perform with the appropriate clinical manifestation or body system:.
Pulse oximetry.
Heart sounds.
Arterial pulses
Skin color, temperature, turgor.
Presence or absence of anxiety.
The Correct Answer is E
The presence or absence of anxiety is a noninvasive assessment that the RN would perform to evaluate the patient’s psychological status and possible signs of hypovolemic shock.
Anxiety can indicate reduced cerebral perfusion due to blood loss and low blood pressure.
Choice A is wrong because pulse oximetry is a noninvasive assessment that the RN would perform to measure the oxygen saturation of the patient’s blood, not the circulatory status.
Choice B is wrong because heart sounds are a noninvasive assessment that the RN would perform to auscultate the cardiac rhythm and rate of the patient, not the circulatory status.
Choice C is wrong because arterial pulses are a noninvasive assessment that the RN would perform to palpate the strength and quality of the patient’s peripheral pulses, not the circulatory status.
Choice D is wrong because skin color, temperature, and turgor are noninvasive assessments that the RN would perform to observe the skin integrity and hydration of the patient, not the circulatory status.
Normal ranges for pulse oximetry are 95% to 100%, for heart rate are 60 to 100 beats per minute, and for blood pressure are 120/80 mmHg.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B"]
Explanation
Pitocin and Methergine are both medications used to manage postpartum hemorrhage (PPH) by causing the uterus to contract and reduce bleeding. Pitocin is the most effective and preferred medication for PPH prevention and treatment.
Choice C is wrong because Terbutaline is a medication that relaxes the uterus and is used to stop preterm labor, not PPH.
Choice D is wrong because Hemabate is a brand name for carboprost, which is a prostaglandin that can be used for PPH, but it has more side effects and contraindications than Pitocin or Methergine.
Choice E is wrong because Magnesium sulfate is a medication that prevents seizures in women with preeclampsia or eclampsia, not PPH.
Correct Answer is C
Explanation
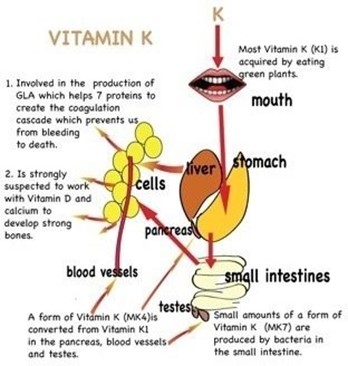
Bacteria that synthesize vitamin K is not present in the newborn’s intestinal tract. Vitamin K is essential for blood clotting, and newborns are at risk of bleeding problems due to their lack of vitamin K. Therefore, vitamin K is given by injection to prevent hemorrhagic disease in the newborn.
Choice A is wrong because most mothers do not have a diet deficient in vitamin K, and vitamin K deficiency in newborns is not related to the maternal diet.
Choice B is wrong because vitamin K does not prevent the synthesis of prothrombin in the liver, but rather enhances it. Prothrombin is a clotting factor that requires vitamin K for its production.
Choice D is wrong because the supply of vitamin K is not inadequate for at least 3 to 4 months, but rather for a few days until the newborn’s intestinal bacteria start producing it.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today