The healthcare provider gives a pregnant woman a prescription for one prenatal vitamin with iron daily and tells her to increase iron-rich foods in her diet because her hemoglobin is 8.2 g/dL or (5.09 mmol/L).
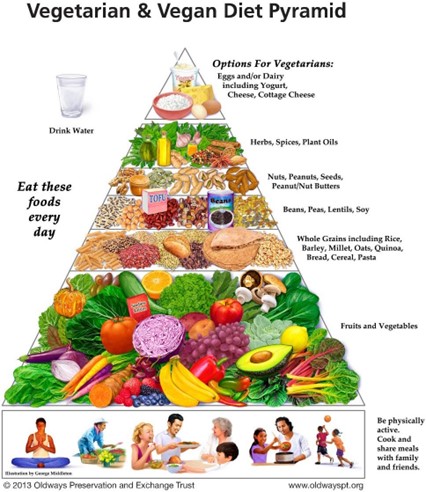
When a list of iron-rich foods is given to the client, she tells the practical nurse (PN) that she is vegetarian and does not eat anything that "bleeds." Which instruction should the PN provide? (Select all that apply.)
Add lentils and black beans to soups
Eat red meat just until the anemia is resolved
Take two prenatal vitamins with iron daily
Oatmeal is a good choice for breakfast
Increase green leafy vegetables in the diet
Correct Answer : A,D,E
Since the pregnant woman is vegetarian and does not eat meat, the practical nurse (PN) should provide alternative sources of iron-rich foods. Lentils and black beans are excellent vegetarian sources of iron and can be added to soups to increase iron intake (option a).
Oatmeal is a good choice for breakfast as it is often fortified with iron (option d). This can help supplement
iron intake in the diet.
Green leafy vegetables, such as spinach, kale, and broccoli, are also rich in iron and should be increased in the client's diet (option e).
Option b, which suggests eating red meat just until the anemia is resolved, is not appropriate for a vegetarian client.
Option c, taking two prenatal vitamins with iron daily, is not necessary unless specifically advised by the healthcare provider. It is important to follow the prescribed dosage of medication and supplements as directed by the healthcare provider.
 |
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
The correct answer is choice c. Ensure that the call bell is easily accessible to the client.
Choice A rationale:
Reassuring the client that someone will check on him hourly is supportive but does not directly address the immediate need for the client to call for assistance if he needs to use the bathroom during the night.
Choice B rationale:
Placing fresh water and a glass within reach is helpful for hydration but may increase the need to urinate, which could exacerbate the issue of urinary frequency at night.
Choice C rationale:
Ensuring that the call bell is easily accessible allows the client to quickly and safely request assistance if he needs to use the bathroom, reducing the risk of falls and ensuring timely help.
Choice D rationale:
Offering an evening snack before providing oral care is a good practice for comfort and nutrition but does not directly address the issue of urinary frequency or the need for nighttime assistance.
Correct Answer is D
Explanation
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today