In caring for the premature infant, the nurse must continually assess hydration status. Parameters to assess would include all of the following except:
Select one:
Daily weight.
Consistency of stool.
Volume of urine output.
Blood pH.
The Correct Answer is D
Choice A Reason: Daily weight. This is an incorrect answer that indicates a valid parameter to assess hydration status. Daily weight is a measure of the body mass that can reflect changes in fluid balance. Daily weight can help detect fluid loss or gain in premature infants, who are more prone to dehydration or overhydration due to immature renal function and high insensible water loss.
Choice B Reason: Consistency of stool. This is an incorrect answer that indicates a valid parameter to assess hydration status. Consistency of stool is a measure of the texture and form of feces that can reflect changes in fluid intake and absorption. Consistency of stool can help identify diarrhea or constipation in premature infants, who are more susceptible to gastrointestinal problems such as necrotizing enterocolitis or feeding intolerance.
Choice C Reason: Volume of urine output. This is an incorrect answer that indicates a valid parameter to assess hydration status. Volume of urine output is a measure of the amount of urine produced and excreted by the kidneys that can reflect changes in fluid balance and renal function. Volume of urine output can help monitor hydration status and kidney function in premature infants, who are more vulnerable to fluid overload or deficit and renal impairment.
Choice D Reason: Blood pH. This is because blood pH is a measure of the acidity or alkalinity of the blood, which reflects the balance between carbon dioxide and bicarbonate in the body. Blood pH is not a direct indicator of hydration status, which refers to the amount of water and electrolytes in the body. Hydration status can affect blood pH, but blood pH can also be influenced by other factors such as respiratory or metabolic disorders.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
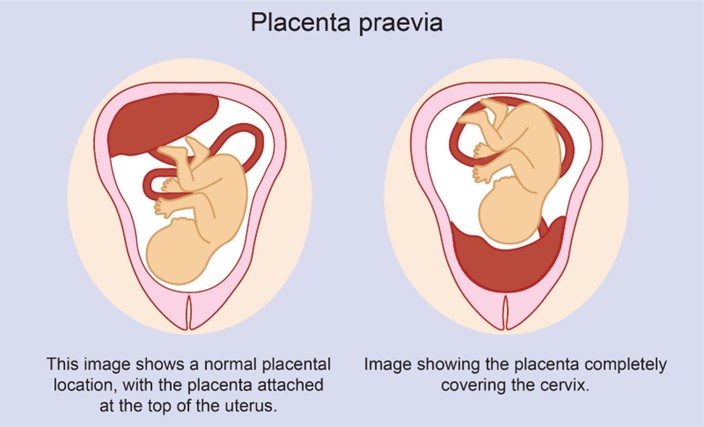
Choice A Reason: Partial placenta previa is a condition where the placenta partially covers the cervix. It usually does not resolve and may cause bleeding and complications during labor and delivery.
Choice B Reason: Complete placenta previa is a condition where the placenta completely covers the cervix. It is a serious condition that requires cesarean delivery and may cause life-threatening hemorrhage.
Choice C Reason: Marginal placenta previa is a condition where the edge of the placenta reaches the margin of the cervix. It may also cause bleeding and complications during labor and delivery.
Choice D Reason: Low-lying placenta previa is a condition where the placenta is near the cervix, but not covering it. It may resolve spontaneously as the uterus grows and the placenta moves upward.
Correct Answer is D
Explanation
Choice A Reason: Apical pulse of 148 beats per minute. This is not a finding that would support a diagnosis of RDS, but rather a normal finding for a newborn. A normal apical pulse for a newborn ranges from 120 to 160 beats per minute. A high pulse rate may indicate fever, infection, anemia, or dehydration. A low pulse rate may indicate hypothermia, hypoxia, or heart block.
Choice B Reason: Respiratory rate of 40 during sleep. This is not a finding that would support a diagnosis of RDS, but rather a normal finding for a newborn. A normal respiratory rate for a newborn ranges from 40 to 60 breaths per minute. A high respiratory rate may indicate respiratory distress, infection, or metabolic acidosis. A low respiratory rate may indicate respiratory depression, hypothermia, or narcotic exposure.
Choice C Reason: Skin color jaundiced. This is not a finding that would support a diagnosis of RDS, but rather a different condition called jaundice. Jaundice is a yellowish discoloration of the skin and mucous membranes caused by elevated levels of bilirubin in the blood. Bilirubin is a breakdown product of hemoglobin that is normally excreted by the liver and kidneys. Jaundice can occur in newborns due to immature liver function, increased red blood cell breakdown, or blood group incompatibility. Jaundice does not affect lung function or oxygenation.
Choice D Reason: Chest retractions. This is because chest retractions are a sign of respiratory distress that indicate increased work of breathing and reduced lung compliance. Chest retractions occur when the chest wall sinks in between the ribs or below the sternum during inhalation, creating a negative pressure that helps draw air into the lungs. RDS is a serious condition where the newborn's lungs are immature and lack sufficient surfactant, which is a substance that reduces surface tension and prevents alveolar collapse. RDS can cause respiratory distress, hypoxia, acidosis, and organ failure. It is more common in preterm infants, especially those born before 37 weeks' gestation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today