When the nurse is assessing a postpartum client approximately 6 hours after delivery, which finding would warrant further investigation?
Select one:
Moderate amounts of deep red lochia.
Sweating while afebrile.
Voiding 350 mL of blood-tinged urine.
Heart rate of 115 beats/minute.
The Correct Answer is D
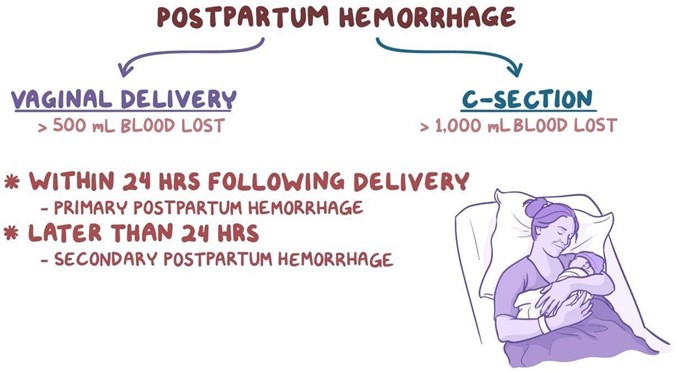
Choice A Reason: Moderate amounts of deep red lochia. This is not a finding that would warrant further investigation, but rather a normal finding for the early postpartum period. Lochia is the vaginal discharge that occurs after delivery, which consists of blood, mucus, and tissue from the uterus. Lochia is usually deep red in color and moderate in amount for the first few days after delivery.
Choice B Reason: Sweating while afebrile. This is not a finding that would warrant further investigation, but rather a common occurrence in the postpartum period. Sweating is a mechanism of thermoregulation that helps the body eliminate excess fluid and electrolytes that were retained during pregnancy. Sweating does not necessarily indicate fever or infection.
Choice C Reason: Voiding 350 mL of blood-tinged urine. This is not a finding that would warrant further investigation, but rather an expected outcome for the postpartum period. Voiding large amounts of urine is normal in the postpartum period, as the body eliminates the excess fluid that was accumulated during pregnancy. Blood-tinged urine may be due to trauma or irritation of the urinary tract during labor or delivery, which usually resolves within a few days.
Choice D Reason: Heart rate of 115 beats/minute. This is because a heart rate of 115 beats/minute is higher than the normal range for an adult, which is 60 to 100 beats/minute. A high heart rate may indicate postpartum hemorrhage, infection, pain, anxiety, or dehydration. The nurse should further assess the client for other signs and symptoms of these conditions and notify the physician if necessary.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: "If I go too long overdue, the amniotic fluid volume can become too low for my baby to be safe." This is a correct answer that indicates that the client understands one of the Reasons for induction of labor at 42 weeks' pregnancy.
Choice B Reason: "My baby took longer to grow, and now she's ready to be born." This is an incorrect answer that shows a misconception about fetal growth and development. Fetal growth does not depend on gestational age alone, but also on genetic, maternal, placental, and environmental factors. A post-term fetus does not necessarily grow faster or larger than a term fetus. In fact, some post-term fetuses may experience intrauterine growth restriction (IUGR), which means slower than expected growth for gestational age.
Choice C Reason: "I don't really need this induction, my baby will come whenever he wants to." This is an incorrect answer that reveals a lack of awareness or acceptance of the need for induction of labor at 42 weeks' pregnancy. Induction of labor is recommended for post-term pregnancies to prevent potential complications such as fetal distress, stillbirth, or maternal hemorrhage.
Choice D Reason: "Since I am so tired of being pregnant, I am being induced." This is an incorrect answer that implies that induction of labor is based on maternal preference or convenience rather than medical indication. Induction of labor should not be done without a valid Reason or informed consent, as it carries some risks such as failed induction, prolonged labor, infection, uterine rupture, or cesarean delivery.
Correct Answer is A
Explanation
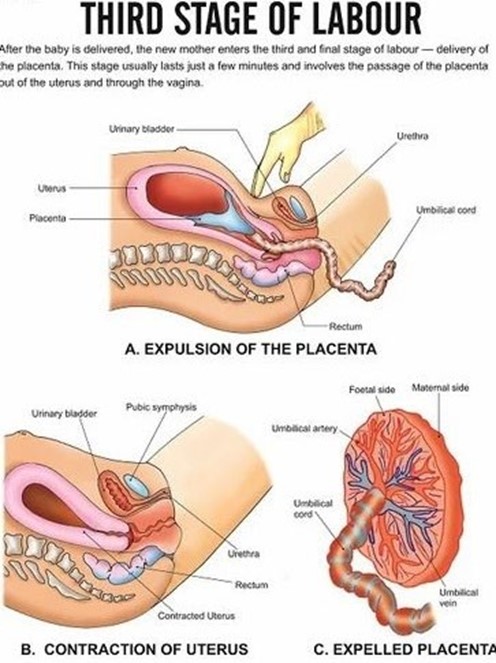
Choice A Reason: Assisting with the delivery of the placenta and ensuring that the fundus is contracted afterward. This is an appropriate action for the nurse to perform during the third stage of labor, as it helps complete the process of labor and prevent complications.
Choice B Reason: Palpating the woman's fundus for position and firmness. This is an action that is done after the delivery of the placenta, not during. It is important to monitor the fundal height, location, and consistency to assess uterine involution and bleeding.
Choice C Reason: Encouraging the woman to push with her contractions. This is an action that is done during the second stage of labor, not the third. The second stage of labor is the period from full cervical dilation to the birth of the baby. The nurse's role is to support and coach the woman to push effectively with her contractions.
Choice D Reason: Alleviating perineal discomfort with the application of ice packs. This is an action that is done after the delivery of the placenta, not during. It is a comfort measure that can reduce swelling, pain, and inflammation in the perineal area.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today