The nurse is caring for a one-month-old infant admitted for suspected congenital hypothyroidism. Which diagnostic test results should the nurse report to the healthcare provider?
Luteinizing hormone (LH) levels.
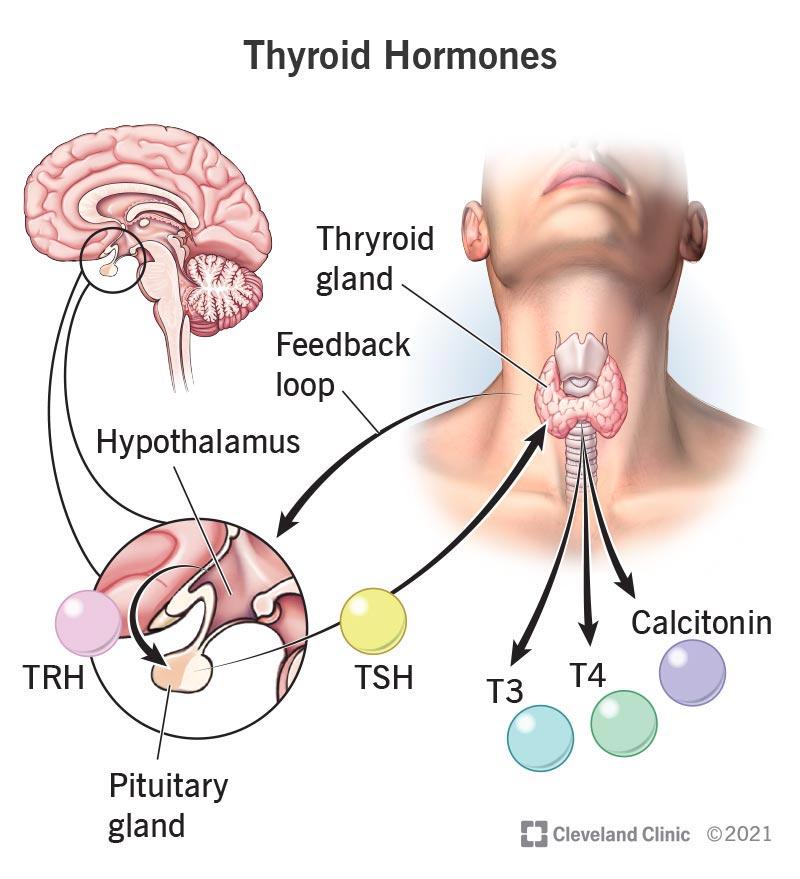
Thyroxine (T4).
Growth hormone (GH) levels.
Follicle stimulating hormone (FSH) levels.
The Correct Answer is B
Choice A reason: Luteinizing hormone (LH) levels are not relevant for the diagnosis of congenital hypothyroidism. LH is a hormone that regulates the reproductive system and is not affected by thyroid function.
Choice B reason: Thyroxine (T4) is the main hormone produced by the thyroid gland and is essential for growth and development. Low levels of T4 indicate hypothyroidism and require treatment with thyroid hormone replacement. High levels of T4 indicate hyperthyroidism and require treatment with anti-thyroid drugs.
Choice C reason: Growth hormone (GH) levels are not relevant for the diagnosis of congenital hypothyroidism. GH is a hormone that stimulates growth and metabolism and is not affected by thyroid function.
Choice D reason: Follicle stimulating hormone (FSH) levels are not relevant for the diagnosis of congenital hypothyroidism. FSH is a hormone that regulates the reproductive system and is not affected by thyroid function.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: Encouraging the parents to rest when possible is not the first intervention that the nurse should instruct the mother to implement. While it is important for the parents to take care of themselves, the priority is to address the child's needs and comfort.
Choice B reason: Making a list of foods that the child likes is not the first intervention that the nurse should instruct the mother to implement. While it is important to maintain the child's nutrition and hydration, the child may not have an appetite due to the fever and inflammation caused by Kawasaki disease.
Choice C reason: Placing the child in a quiet environment is the first intervention that the nurse should instruct the mother to implement. This is because Kawasaki disease causes irritability and sensitivity to light and sound in the child. A quiet environment can help reduce the child's stress and discomfort.
Choice D reason: Applying lotion to hands and feet is not the first intervention that the nurse should instruct the mother to implement. While it is important to moisturize the skin and prevent cracking and infection, the lotion may not relieve the child's pain and inflammation.
Correct Answer is A
Explanation
Choice A reason: The lumen of the aorta reduces the volume of blood flow to the lower extremities is the correct pathophysiologic mechanism that supports the findings. This is because coarctation of the aorta is a congenital condition that causes a narrowing of the aorta, usually near the ductus arteriosus. This results in increased resistance to blood flow from the heart to the lower body, leading to higher blood pressure and stronger pulses in the upper extremities and lower blood pressure and weaker pulses in the lower extremities.
Choice B reason: The aortic semilunar valve obstructs blood flow into the systemic circulation is not the correct pathophysiologic mechanism that supports the findings. This is because the aortic semilunar valve is located at the base of the aorta and prevents blood from flowing back into the left ventricle. If the valve is obstructed, it would cause aortic stenosis, which is a different condition from coarctation of the aorta. Aortic stenosis would cause symptoms such as chest pain, shortness of breath, and fainting.
Choice C reason: The pulmonic valve prevents adequate blood volume into the pulmonary circulation is not the correct pathophysiologic mechanism that supports the findings. This is because the pulmonic valve is located at the base of the pulmonary artery and prevents blood from flowing back into the right ventricle. If the valve is obstructed, it would cause pulmonic stenosis, which is a different condition from coarctation of the aorta. Pulmonic stenosis would cause symptoms such as cyanosis, fatigue, and heart murmur.
Choice D reason: An opening in the atrial septum causes a murmur due to a turbulent left to right shunt is not the correct pathophysiologic mechanism that supports the findings. This is because an opening in the atrial septum is a defect in the wall that separates the two upper chambers of the heart. It would cause a condition called atrial septal defect, which is different from coarctation of the aorta. Atrial septal defect would cause symptoms such as difficulty breathing, frequent respiratory infections, and heart palpitations.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today