The nurse is performing an admission assessment for a newborn who has asymmetrical buttocks. Which assessment test results should the nurse report to the healthcare provider?
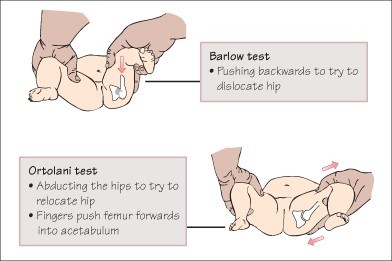
Ortolani maneuver causing a click at the hip joint.
Plumb line test indicates fetal position curvature.
Babinski test that reveals fanning out of toes.
Moro test precipitating a startle response.
The Correct Answer is A
The Ortolani maneuver is a physical examination technique used to assess for developmental dysplasia of the hip (DDH) in newborns. During the maneuver, the nurse gently abducts the infant's hips and applies gentle pressure to detect any instability or "click" at the hip joint. A positive Ortolani maneuver, where a click or clunk is felt or heard, can indicate the presence of a hip dislocation or dysplasia.
Asymmetrical buttocks can be a sign of hip dysplasia in newborns, and a positive Ortolani maneuver is an important finding that suggests a potential hip joint problem. Reporting this assessment test result to the healthcare provider allows for further evaluation and appropriate management of the newborn's hip condition.
The Plumb line test, which assesses fetal position curvature, is not directly related to hip dysplasia and may not be significant in this context.
The Babinski test, which reveals fanning out of the toes, is used to assess the integrity of the infant's neurological system and is not specific to hip dysplasia.
The Moro test, also known as the startle response, is a reflex assessment used to evaluate the newborn's neurological and sensory function. While it is important to assess the overall neurological status of the newborn, the Moro test is not specific to hip dysplasia.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","D","E"]
Explanation
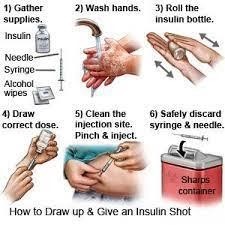
A) Correct - Demonstrating the technique used to monitor blood glucose levels is crucial.
Incorrect technique can lead to inaccurate readings, impacting insulin dosing decisions and blood sugar control.
B) Correct - Some asthma medications, like corticosteroids, can elevate blood glucose levels.
Evaluating the client's asthma medications is essential as they can contribute to fluctuations in blood sugar levels.
C) Incorrect- Asking the client if they want a different manufacturer's glucose monitoring device is not helpful, because it does not address the underlying causes of the poor glycemic control. The client may also perceive this as a lack of confidence in their ability to manage their diabetes or as a criticism of their choice of device. The nurse should focus on educating the client on how to use their current device correctly and consistently, rather than suggesting a change that may not be necessary or feasible.
D) Correct - Understanding the client's daily routine helps identify factors influencing blood glucose control, such as meal timing, activity level, and stress. This information aids in creating a personalized diabetes management plan.
E) Correct - Ensuring the client uses a new insulin needle for each administration is important for preventing infection and complications. Reusing needles can affect injection site health and insulin absorption.
Correct Answer is C
Explanation
Given the client's symptoms of constant chest pressure that is unrelieved with rest, along with the client's appearance of anxiety, pallor, and diaphoresis, it indicates a high likelihood of an acute coronary event, such as a myocardial infarction (heart attack). In this situation, the nurse should prioritize immediate actions that address the potential cardiac emergency.
Aspirin is an essential medication in the initial management of acute coronary syndrome, including unstable angina and myocardial infarction. It helps to inhibit platelet aggregation and reduce the risk of clot formation in the coronary arteries. The chewable form of aspirin is recommended because it allows for more rapid absorption.
While evaluating extremities for perfusion, pulse volume, and pitting edema is important in assessing the client's overall cardiovascular status, it is not the immediate next step when faced with a suspected acute coronary event.
Securing client consent for coronary angiography and percutaneous coronary intervention (PCI) is a relevant step in the management of unstable angina and myocardial infarction, but it is not the immediate action to be taken in the emergency department. The client requires stabilization and initial medical interventions before procedural consent can be obtained.
Placing an indwelling urinary catheter and instituting strict intake and output measurements is not a priority action in this situation. The focus should be on addressing the potential acute coronary event and ensuring the client's cardiac stability. Urinary catheterization and monitoring of intake and output can be considered later, if necessary.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today