Which health care provider prescription for a client with a nephrostomy tube should a nurse question?
Monitor the urine’s color and odor.
Record the intake and output every eight hours.
Irrigate the tube with 30 mL of sterile saline as needed.
Measure the vital signs every four hours during the day.
The Correct Answer is C
Irrigating the tube with 30 mL of sterile saline as needed. This prescription should be questioned by the nurse because it may cause trauma to the kidney or dislodge the tube. The nurse should only irrigate the tube if ordered by the health care provider and with a smaller amount of fluid.
Choice A is wrong because monitoring the urine’s color and odor is an appropriate intervention for a client with a nephrostomy tube. The urine may be bloody or cloudy initially, but it should gradually clear.
Choice B is wrong because recording the intake and output every eight hours is also an appropriate intervention for a client with a nephrostomy tube. The nurse should measure and document the amount and characteristics of urine drainage and report any changes or abnormalities.
Choice D is wrong because measuring the vital signs every four hours during the day is a reasonable prescription for a client with a nephrostomy tube. The nurse should monitor the client for signs of infection, bleeding, or obstruction.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Rhonchi. Rhonchi are low-pitched, rattling sounds that indicate mucus in the larger airways. They are most evident on expiration and may decrease after coughing.
Choice B is wrong because wheezes are high-pitched, squeaking sounds that indicate narrowed small air passages. They are usually heard on both inspiration and expiration.
Choice C is wrong because crackles are short, high-pitched popping sounds that indicate fluid or inflammation in the alveoli. They are usually heard on inspiration.
Choice D is wrong because pleural friction rubs are creaking or grating sounds that indicate inflammation of the pleura. They are usually heard on both inspiration and expiration and do not change with coughing.
Correct Answer is A
Explanation
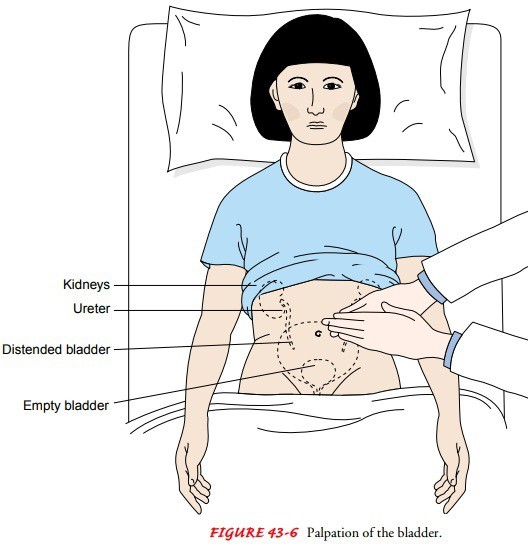
The nurse should first assess the client’s bladder for distention by palpating the lower abdomen between the symphysis pubis and the umbilicus.
This can indicate urinary retention, which is a common postoperative complication. The nurse should also measure the bladder volume using a bladder scanner if available.
Choice B. Inform the surgeon that the client’s status is wrong because the nurse should first assess the client before notifying the surgeon.
The surgeon may order interventions based on the assessment findings.
Choice C. Increasing the client’s fluid intake is wrong because increasing fluid intake may worsen bladder distention and discomfort.
The nurse should encourage fluid intake only after ensuring adequate urinary output.
Choice D. Administering pain medication is wrong because pain medication may not be indicated for urinary retention.
Pain medication may also cause urinary retention by relaxing the bladder muscles and impairing the micturition reflex.
Normal urine output is about 30 mL per hour or 240 mL in eight hours.
The nurse should monitor the client’s intake and output and report any signs of urinary retention to the surgeon.
Urinary retention can lead to infection, bladder damage, and renal impairment if not treated promptly.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today