Which modification is usually tried first when a child is diagnosed with juvenile idiopathic arthritis (JI
Aspirin
Corticosteroids
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Disease Modifying Anti-Rheumatoid Drugs (DMARDs)
The Correct Answer is C
The correct answer is c. Nonsteroidal anti-inflammatory drugs (NSAIDs)
Choice A reason:
Aspirin was once commonly used to treat juvenile idiopathic arthritis (JIA), but it is no longer the first-line treatment due to its potential side effects, such as gastrointestinal issues and Reye’s syndrome in children. While it can still be used in some cases, it is not the preferred initial treatment.
Choice B Reason:
Corticosteroids are effective in reducing inflammation and controlling symptoms of JIA, but they are not typically used as the first-line treatment due to their potential side effects, including weight gain, growth suppression, and increased risk of infections. They are usually reserved for more severe cases or when other treatments have failed.
Choice C Reason:
Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first-line treatment for juvenile idiopathic arthritis. They help reduce inflammation, relieve pain, and improve joint function. NSAIDs are generally well-tolerated and have a long track record of safety and effectiveness in managing JIA.
Choice D Reason:
Disease Modifying Anti-Rheumatoid Drugs (DMARDs), such as methotrexate, are used in the treatment of JIA, but they are not typically the first-line treatment. DMARDs are often prescribed when NSAIDs are not sufficient to control the symptoms or when the disease is more severe. They help slow the progression of the disease and prevent joint damage.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
The correct answer is a) Androgens.
Choice A reason:
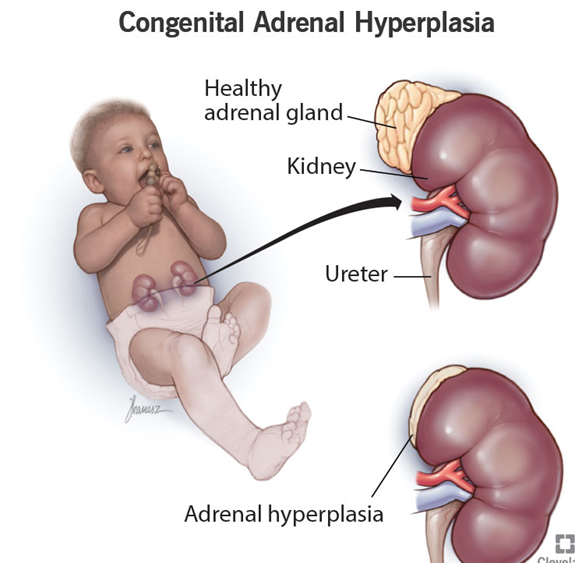
Congenital adrenal hyperplasia (CAH) is a group of genetic disorders affecting the adrenal glands, which are responsible for producing vital hormones such as cortisol, aldosterone, and androgens. In CAH, there is a deficiency of the enzyme 21-hydroxylase, which is crucial for the synthesis of cortisol and aldosterone. As a result, the adrenal glands overproduce androgens, leading to symptoms such as ambiguous genitalia in newborns, early puberty, and rapid growth. Androgens are male sex hormones, including testosterone, which play a significant role in the development of male characteristics.
Choice B reason:
Vitamin K is a fat-soluble vitamin essential for blood clotting and bone health. It is not related to the overproduction of hormones in congenital adrenal hyperplasia. Vitamin K deficiency can lead to bleeding disorders, but it does not cause the symptoms associated with CAH, such as ambiguous genitalia or early puberty. Therefore, this choice is incorrect.
Choice C reason:
Gonadotropins are hormones produced by the pituitary gland that stimulate the gonads (ovaries and testes) to produce sex hormones and gametes (eggs and sperm). While gonadotropins play a role in sexual development and reproduction, they are not overproduced in congenital adrenal hyperplasia. The primary issue in CAH is the overproduction of androgens due to enzyme deficiencies in the adrenal glands. Therefore, this choice is incorrect.
Choice D reason:
Vitamin D is a fat-soluble vitamin essential for calcium absorption and bone health. It is not related to the overproduction of hormones in congenital adrenal hyperplasia. Vitamin D deficiency can lead to bone disorders such as rickets in children and osteomalacia in adults, but it does not cause the symptoms associated with CAH. Therefore, this choice is incorrect.
Correct Answer is D
Explanation
The correct answer is d) Recurrent kidney infections.
Choice A reason:
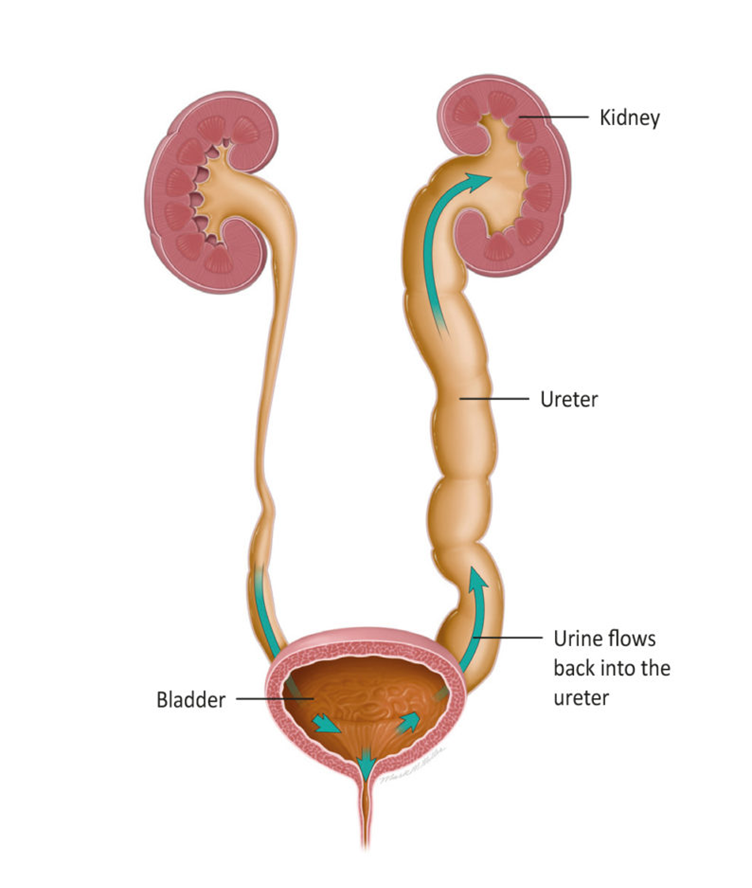
Infarction of the renal vessels is not a common consequence of vesicoureteral reflux (VUR). Infarction refers to tissue death due to a lack of blood supply, which is not typically associated with VUR1. VUR primarily affects the urinary tract, leading to the backward flow of urine from the bladder into the ureters and kidneys. This condition can cause other complications, but infarction of the renal vessels is not one of them.
Choice B reason:
Renal calculi, or kidney stones, are not directly caused by vesicoureteral reflux. While VUR can lead to urinary tract infections (UTIs), which may increase the risk of developing kidney stones, it is not the primary outcome. Kidney stones are typically formed due to an imbalance of minerals and salts in the urine, leading to crystallization. VUR itself does not directly cause the formation of renal calculi.
Choice C reason:
Urinary obstruction is not a typical result of vesicoureteral reflux. VUR involves the backward flow of urine, but it does not usually cause a physical blockage in the urinary tract. Urinary obstruction can occur due to other conditions, such as congenital abnormalities, tumors, or kidney stones, but it is not a direct consequence of VUR.
Choice D reason:
Recurrent kidney infections are a common complication of vesicoureteral reflux. The backward flow of urine can carry bacteria from the bladder into the kidneys, leading to repeated episodes of pyelonephritis (kidney infection). These recurrent infections can cause kidney damage over time if not properly managed. Therefore, it is crucial to monitor and treat VUR to prevent recurrent kidney infections and preserve kidney function.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today