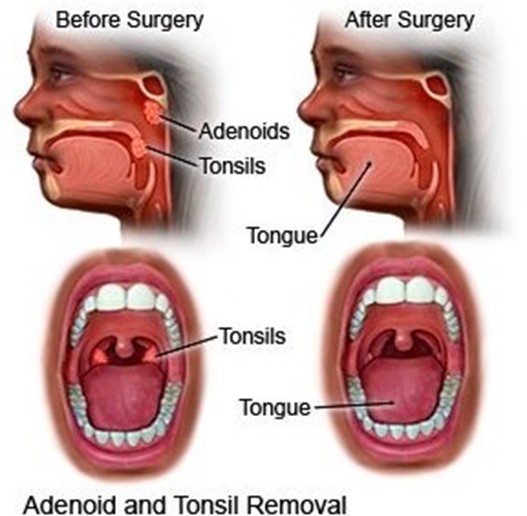
While obtaining the vital signs of a 10-year-old child who had a tonsillectomy this morning, the nurse observes the child swallowing every 2 to 3 minutes.
Which assessment should the nurse implement?
Inspect the posterior oropharynx.
Touch the tonsillar pillars to stimulate the gag reflex.
Ask the child to speak to evaluate change in voice tone.
Assess for teeth clenching or grinding.
The Correct Answer is A
The nurse should inspect the posterior oropharynx of a child who is frequently swallowing after tonsillectomy to assess for bleeding or the presence of clots. Swallowing frequently can be a sign of postoperative bleeding, which is a potential complication of tonsillectomy.
Touching the tonsillar pillars to stimulate the gag reflex or asking the child to speak would not provide information about the presence of bleeding.
Assessing for teeth clenching or grinding is not related to this particular observation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
If a child's systolic blood pressure is greater than the 90th percentile during a routine clinic visit, the nurse should take the blood pressure two more times during the visit and determine the average of the three readings. This will provide a more accurate assessment of the child's blood pressure. Referring the child to the healthcare provider and scheduling an evaluation of blood pressure in two weeks
A. may be necessary if the child's blood pressure remains elevated, but it is not the next action that should be taken. Measuring the child's blood pressure three times during the visit and determining the highest of the readings
B. is not recommended because it may overestimate the child's blood pressure. Conducting a head-to-toe assessment and omitting repeated blood pressures during the examination
C. is not appropriate because it does not provide an accurate assessment of the child's blood pressure.
Correct Answer is B
Explanation
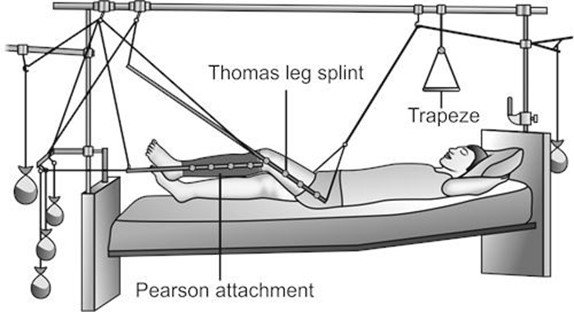
When caring for a child in balanced suspension skeletal traction, the most important intervention for the nurse to implement is monitoring peripheral pulses and sensation in the affected leg to detect any compromise in circulation or nerve function. This is crucial because the traction places tension on the bones, which can result in nerve or vascular damage.
Changing positions every 2 hours is important to prevent pressure injuries, but it is not the most critical intervention.
Cleansing pin sites and assessing skin for redness and signs of tissue breakdown are also important, but they are not as urgent as monitoring peripheral pulses and sensation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today