
Ati en300 med surg Exam
Ati en300 med surg Exam
Total Questions : 53
Showing 10 questions Sign up for moreTo properly identify a cardiac rhythm, the nurse will determine if the client's rhythm contains the following factors: (Select All that Apply.)
Explanation
A. The P-P and R-R distances are equal and regular: Equal and regular spacing between P-P and R-R intervals indicates that both atrial and ventricular rhythms are regular. This is a fundamental aspect of rhythm interpretation, helping to distinguish between regular and irregular rhythms such as atrial fibrillation or sinus arrhythmia.
B. The rhythm rate using a 3-second strip: Assessing the heart rate using a 3-second or 6-second ECG strip helps determine whether the rhythm is bradycardic, tachycardic, or within normal limits, which is crucial for accurate rhythm classification.
C. The duration of the U waves: U waves are typically small and follow the T wave. Although their presence can suggest conditions like hypokalemia, they are not routinely assessed in basic rhythm identification. Evaluating U wave duration is more relevant in electrolyte imbalance analysis than in identifying rhythm type.
D. There is a QRS complex after each P wave: A consistent QRS following every P wave indicates effective conduction from the atria to the ventricles. Each atrial depolarization (P wave) should be followed by a ventricular depolarization (QRS complex) if the signal is being conducted properly through the AV node. This finding supports a diagnosis of sinus rhythm and helps rule out AV blocks, where conduction may be delayed or blocked entirely.
E. P waves are present, upright and rounded: P waves that are upright and rounded in lead II suggest the electrical impulse is originating from the SA node. Their presence and morphology are essential criteria for identifying sinus rhythm and differentiating it from atrial arrhythmias like flutter or fibrillation.
The nurse identifies the following rhythm on the cardiac monitor. Which treatment modality will the nurse anticipate for this client?

Explanation
A. Radiofrequency ablation: This is used to treat tachyarrhythmias such as atrial fibrillation, atrial flutter, or supraventricular tachycardia (SVT). The ECG shown does not demonstrate any tachycardic rhythm rather, it shows a bradyarrhythmia with dropped QRS complexes, which suggests a conduction block, not a reentrant circuit.
B. Administration of amiodarone: Amiodarone is primarily used for ventricular arrhythmias or atrial fibrillation. It is not effective in treating bradyarrhythmias or heart blocks such as those seen in this rhythm strip.
C. Insertion of a pacemaker: The rhythm strip shows intermittent dropped QRS complexes with consistent P waves—this is indicative of second-degree AV block, Mobitz II. This type of conduction block can progress to complete heart block and is often treated with the insertion of a permanent pacemaker to maintain cardiac output.
D. Administration of adenosine: Adenosine is used to terminate SVT by temporarily blocking AV node conduction. It is contraindicated in heart blocks, especially Mobitz II or third-degree AV block, because it can worsen the block and cause asystole.
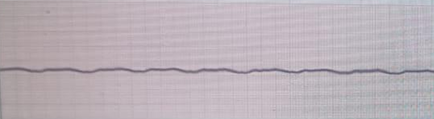
The nurse is caring for a client during a cardiac arrest. The monitor displays the rhythm below. Which intervention should the nurse perform at this time?
Explanation
A. Administer amiodarone 200 mg IV push: Amiodarone is used for shockable rhythms like ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) that are refractory to defibrillation. The rhythm on the monitor is asystole, which is non-shockable, and amiodarone is not indicated here.
B. Defibrillate the client using 200 joules: Defibrillation is only appropriate for shockable rhythms such as VF or pulseless VT. Asystole is not shockable, and defibrillation in this rhythm would be ineffective and inappropriate.
C. CPR until the physician stops the code: The rhythm strip shows asystole, a flatline with no electrical activity. The priority intervention is to initiate and continue high-quality cardiopulmonary resuscitation (CPR) immediately and continue until the code is terminated by the physician. This is consistent with Advanced Cardiac Life Support (ACLS) guidelines.
D. Administer adenosine 12 mg IV push: Adenosine is used to terminate supraventricular tachycardia (SVT) and is not indicated in asystole or during cardiac arrest. It would have no effect in a rhythm with no electrical activity.
A client has been admitted to the Post Anesthesia Care Unit (PACU) after a completing electroconvulsant therapy (ECT) treatment. Which action will the nurse perform first?
Explanation
A. Assist the client from the stretcher to a wheelchair: Immediately after electroconvulsive therapy (ECT), the client is still recovering from anesthesia and may experience confusion, drowsiness, or muscle weakness. Transferring the client prematurely poses a fall risk and is not appropriate as the first action.
B. Orient the client and offer reassurance: While reorientation and reassurance are important aspects of post-ECT care, safety and physiological stability must be assessed first. This action should follow an initial assessment of vital signs and level of consciousness.
C. Encourage the client to drink some fluids: Offering fluids too soon after ECT is inappropriate because the client may have impaired swallowing reflexes from anesthesia or sedation. Ensuring the airway is clear and the client is fully alert must precede oral intake.
D. Assess vital signs and orient client to the PACU environment: The priority after any procedure involving anesthesia is to assess vital signs to ensure hemodynamic stability and monitor for complications. Once stable, the nurse can begin to orient the client, which is often needed after ECT due to temporary disorientation or memory lapses.
The nurse observes the following rhythm of a client on the telemetry unit. Which action should be completed first?

Explanation
A. Administer amiodarone IV push followed by a continuous infusion: Amiodarone is part of the Advanced Cardiac Life Support (ACLS) algorithm for ventricular fibrillation (VF) or pulseless ventricular tachycardia, but it should only be given after confirming the rhythm and initiating basic life support steps, including pulse check.
B. Establish unresponsiveness and check the carotid pulse: The rhythm strip shows ventricular fibrillation, a life-threatening arrhythmia. However, before initiating advanced interventions such as defibrillation, the nurse must first confirm the client is unresponsive and pulseless, which is the correct initial action according to ACLS protocols.
C. Immediately defibrillate the client using the synchronous mode: Defibrillation is the correct treatment for VF, but it must be done in unsynchronized mode. Additionally, it is not appropriate to defibrillate until pulselessness is confirmed. Synchronized mode is used for rhythms like unstable SVT or atrial fibrillation not VF.
D. Initiate a rapid response call and increase the monitor’s sensitivity: A rapid response team is called for deteriorating patients who are still responsive. If the client is unresponsive and pulseless, a code blue or cardiac arrest protocol should be initiated, not just a rapid response. Monitor sensitivity adjustments are irrelevant in a confirmed life-threatening rhythm.
A client is to receive an intravenous dose of adenosine. What immediate response to this medication should the nurse expect?
Explanation
A. Run of premature ventricular beats: While adenosine can occasionally provoke brief ventricular ectopy, this is not its primary or most expected effect. Premature ventricular contractions may occur transiently but are not the hallmark response to this medication.
B. Short period of asystole: Adenosine briefly blocks AV node conduction and can interrupt re-entry pathways, often resulting in a short period of asystole lasting a few seconds. This is an expected effect and reflects the drug’s mechanism in terminating supraventricular tachycardia by interrupting the reentrant pathway.
C. Brief seizure episode: Adenosine does not typically cause seizures. It acts primarily on cardiac tissue and has no significant pro-convulsant effects. A seizure would be an atypical and concerning adverse reaction rather than an expected response.
D. Dramatic increase in blood pressure: Adenosine causes transient vasodilation and may lead to a brief drop in blood pressure or flushing. A dramatic increase in blood pressure would not be expected and could suggest an alternate diagnosis or drug reaction.
The nurse is caring for a client in the coronary care unit and the monitor depicts the rhythm shown below. What is the nurse's interpretation of this rhythm?

Explanation
A. Sinus Bradycardia, with First Degree AV block, Rate 40: The rhythm strip shows regular P waves, each followed by a QRS complex, indicating a sinus rhythm. The PR interval is prolonged (greater than 0.20 seconds) but remains consistent across all beats. This confirms a first-degree AV block. The ventricular rate is approximately 40 bpm, consistent with sinus bradycardia.
B. Second Degree AV block – Mobitz I, Rate 40: Mobitz I (Wenckebach) is characterized by a progressively lengthening PR interval followed by a dropped QRS complex. This pattern is not seen here; the PR intervals are consistently prolonged.
C. Second Degree AV block – Mobitz II, Rate 40: Mobitz II involves intermittent dropped QRS complexes without progressive PR prolongation. In the strip, no QRS complexes are missing, ruling out Mobitz II.
D. Third Degree Heart Block, Rate 40: In complete heart block, there is no relationship between P waves and QRS complexes (AV dissociation). Here, the P waves are consistently followed by QRS complexes, indicating intact conduction, even if delayed. This therefore is not a third-degree block.
The nurse understands that sinus tachycardia differs from normal sinus rhythm because:
Explanation
A. the heart rate is greater than 100 bpm in sinus tachycardia: Normal Sinus Rhythm is characterized by a heart rate between 60 and 100 beats per minute (bpm). Sinus tachycardia is defined as a sinus rhythm with a heart rate exceeding 100 beats per minute. The rhythm remains regular, with each P wave followed by a QRS complex, but the rate is significantly faster than normal sinus rhythm.
B. more p waves are present than QRS complexes: In sinus tachycardia, the number of P waves and QRS complexes remains one-to-one, as each atrial impulse continues to be conducted to the ventricles. More P waves than QRS complexes typically suggest atrial flutter or other forms of AV dissociation.
C. the QRS complexes measure greater than 0.10: A widened QRS complex suggests a bundle branch block or ventricular rhythm, not sinus tachycardia. In sinus tachycardia, QRS complexes typically remain narrow, measuring less than 0.10 seconds unless an intraventricular conduction delay is present.
D. the rhythm is often irregular in sinus tachycardia: Sinus tachycardia is usually a regular rhythm with consistent R-R intervals. An irregular rhythm is more indicative of atrial fibrillation or sinus arrhythmia, not a defining characteristic of sinus tachycardia.
The nurse is caring for a client in the telemetry unit and notices the rhythm below. The client is unresponsive and pulseless. After calling for assistance, what should be the nurse's next action?

Explanation
A. Cardiovert in the synchronized mode: Synchronized cardioversion is used for hemodynamically unstable but conscious patients with rhythms like atrial fibrillation or supraventricular tachycardia. It is not appropriate for a pulseless patient with ventricular fibrillation, as synchronization requires detectable R-waves.
B. Defibrillate immediately with a biphasic machine: The rhythm strip shows ventricular fibrillation (VF) a life-threatening arrhythmia characterized by chaotic, irregular waveform with no identifiable PQRST and no effective cardiac output. The patient is unresponsive and pulseless, making immediate defibrillation the priority action, as per Advanced Cardiac Life Support (ACLS) guidelines.
C. Take a full set of vital signs: The client is already unresponsive and pulseless, making a full set of vitals irrelevant at this moment. Immediate resuscitation efforts, including defibrillation and CPR, take priority.
D. Initiate cardiopulmonary resuscitation: While CPR is a critical part of the algorithm for pulseless rhythms, defibrillation is the first priority in ventricular fibrillation when a defibrillator is available and ready. CPR should be started immediately after the shock if no pulse returns.
The nurse is caring for a client immediately following the insertion of a permanent pacemaker. Which intervention should be included in the plan of care?
Explanation
A. Teach the client how to change the pacemaker dressing: Client education is important but not a priority in the immediate post-procedure phase. Dressing changes should initially be performed using sterile technique by clinical staff to prevent infection at the insertion site.
B. Immobilize the affected arm using a sling: After pacemaker insertion, the affected arm (usually on the side of the implantation) should be immobilized or limited in movement to prevent lead dislodgment. Elevating the arm above the shoulder or excessive motion can compromise pacemaker lead placement during the early healing period.
C. Arrange for ancillary personnel to feed the client: Assistance with feeding is only necessary if the client has physical or cognitive limitations. This is not a routine or priority intervention following pacemaker insertion unless clinically indicated by other assessments.
D. Monitor urine output every two hours: Frequent monitoring of urine output is not directly related to pacemaker insertion unless there are other concerns such as fluid imbalance or renal dysfunction. It's not a standard intervention in the immediate care plan for this procedure.
You just viewed 10 questions out of the 53 questions on the Ati en300 med surg Exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

