A client has not voided eight hours after surgery and says to the nurse, “I don’t think I can urinate.” What should be the first action for the nurse?
Assess the client’s bladder.
Administer pain medication.
Increase the client’s fluid intake.
Inform the surgeon of the client’s status.
The Correct Answer is A
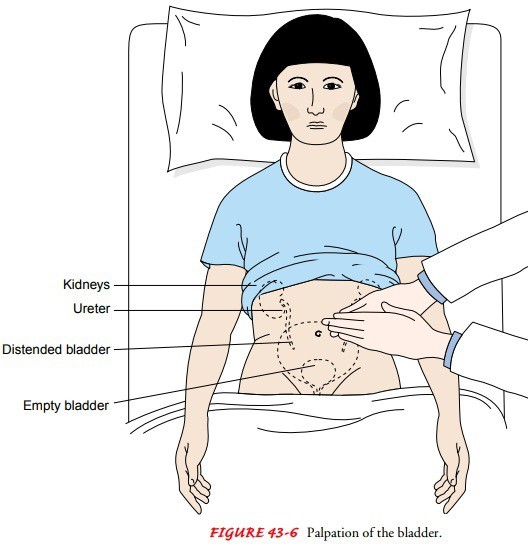
The nurse should first assess the client’s bladder for distention by palpating the lower abdomen between the symphysis pubis and the umbilicus.
This can indicate urinary retention, which is a common postoperative complication. The nurse should also measure the bladder volume using a bladder scanner if available.
Choice B. Inform the surgeon that the client’s status is wrong because the nurse should first assess the client before notifying the surgeon.
The surgeon may order interventions based on the assessment findings.
Choice C. Increasing the client’s fluid intake is wrong because increasing fluid intake may worsen bladder distention and discomfort.
The nurse should encourage fluid intake only after ensuring adequate urinary output.
Choice D. Administering pain medication is wrong because pain medication may not be indicated for urinary retention.
Pain medication may also cause urinary retention by relaxing the bladder muscles and impairing the micturition reflex.
Normal urine output is about 30 mL per hour or 240 mL in eight hours.
The nurse should monitor the client’s intake and output and report any signs of urinary retention to the surgeon.
Urinary retention can lead to infection, bladder damage, and renal impairment if not treated promptly.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A client who grimaces during a dressing change is showing a nonverbal sign of pain. Grimacing is an expression of facial muscles that indicates discomfort or distress.
The nurse should record this as a symptom of pain and ask the client to rate the pain using a numeric or visual scale.
Choice B is wrong because an elevated heart rate while exercising is not necessarily a symptom of pain. It could be a normal response to increased physical activity or a sign of other conditions such as anxiety, dehydration, or fever.
Choice C is wrong because crying during a procedure is not a reliable indicator of pain. Crying is an emotional response that can be influenced by many factors such as fear, stress, or sadness.
The nurse should not assume that the client is in pain based on crying alone and should ask the client about the reason for crying and the level of pain.
Choice D is wrong because saying “I feel achy all over” is not a specific description of pain.
Aching is a vague term that can refer to different sensations such as soreness, stiffness, or cramping.
The nurse should ask the client to clarify what kind of pain they are feeling, where it is located, how severe it is, and what makes it better or worse.
Correct Answer is B
Explanation
A client who has been NPO for four days is most at risk to develop skin breakdown. This is because being NPO (nothing by mouth) can lead
to malnutrition and dehydration, which are both risk factors for bedsores. Malnutrition can impair the skin’s ability to heal and resist infection, while dehydration can make the skin dry and fragile.
Choice A is wrong because applying powder after drying the skin can help prevent moisture and friction, which are also risk factors for bedsores.
Choice C is wrong because bathing twice a week may not be frequent enough to keep the skin clean and free of irritants, which can also contribute to bedsores.
Choice D is wrong because hypertension (high blood pressure) does not directly cause bedsores, although it may be associated with other conditions that affect blood circulation and tissue oxygenation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today