A client, scheduled for open-heart surgery, expresses a desire not to be resuscitated if they pass away during the procedure.
What is the nurse’s subsequent course of action?
Administer the prescribed oral and intravenous pre-operative medications.
Inform the physician after the surgical procedure is complete.
Record and have a clear conversation with the client about their wishes regarding Cardio-Pulmonary Resuscitation.
Verbally communicate the client’s wishes to the supervisor of the operating room.
The Correct Answer is C
Choice A rationale:
Administering pre-operative medications does not address the client's expressed desire regarding resuscitation. It is a necessary step in preparing the client for surgery, but it does not directly relate to their preferences for end-of-life care.
Fulfilling this task does not ensure that the client's wishes are communicated to the appropriate healthcare providers, potentially leading to unwanted resuscitative efforts if the client's condition deteriorates during surgery.
It is crucial for the nurse to prioritize the client's autonomy and right to self-determination regarding their healthcare choices.
Choice B rationale:
Informing the physician after the surgery is complete is not timely and could result in the client's wishes not being respected.
The physician needs to be aware of the client's resuscitation preferences before the procedure begins to ensure that care aligns with their wishes.
Delaying communication could lead to ethical and legal dilemmas if resuscitation is attempted against the client's expressed desires.
Choice C rationale:
This is the most appropriate action because it directly addresses the client's concerns and ensures that their wishes are documented and communicated effectively.
Having a clear conversation with the client allows for exploration of their understanding of resuscitation and any potential concerns or questions they may have.
Recording the client's wishes in their medical record provides a clear record for all healthcare providers involved in their care, promoting consistency and respect for their autonomy.
Choice D rationale:
While verbally communicating the client's wishes to the operating room supervisor is important, it is not sufficient on its own.
Written documentation in the medical record is essential to ensure that the information is accurately conveyed to all members of the healthcare team and accessible throughout the client's care journey.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale:
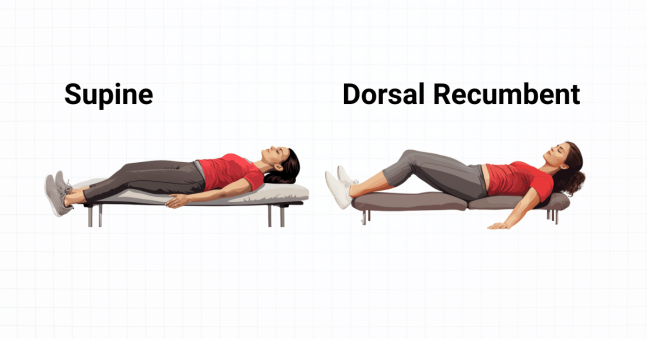
Sims' position is a side-lying position with the lower leg flexed and the upper leg extended. It is not ideal for bladder scanning because it can compress the bladder and make it difficult to obtain an accurate reading.
Additionally, in Sims' position, the bladder may not be fully accessible to the scanner, as it may be partially obscured by the upper thigh.
Choice B rationale:
Dorsal recumbent position is the optimal position for bladder scanning. In this position, the client lies flat on their back with their knees bent and their feet flat on the bed. This position allows for:
Full exposure of the bladder, making it easily accessible to the scanner.
Relaxation of the abdominal muscles, which can help to ensure an accurate reading.
A comfortable position for the client, promoting cooperation and reducing the likelihood of movement that could interfere with the scan.
Choice C rationale:
Supine position is a similar position to dorsal recumbent, but with the legs fully extended. While it is possible to perform a bladder scan in this position, it is not as ideal as dorsal recumbent because:
The extended legs can place some tension on the abdominal muscles, potentially affecting bladder position and the scan's accuracy.
The client may find this position less comfortable, leading to restlessness and potential movement that could interfere with the scan.
Choice D rationale:
High Fowler's position is a semi-sitting position with the head of the bed elevated at a 45- to 60-degree angle. This position is not suitable for bladder scanning because:
Gravity can pull the bladder downwards, making it difficult to visualize and measure accurately.
It can be challenging to maintain proper positioning of the scanner on the abdomen in this position, potentially leading to inaccurate readings.
Correct Answer is ["65"]
Explanation
Here are the steps to calculate the flow rate in gtt/min:
Step 1: Calculate the total volume of fluid to be infused.
The order is for 1.5 grams of Ampicillin added to 100 mL of Normal Saline, so the total volume is 100 mL. Step 2: Calculate the number of vials of Ampicillin needed.
Each vial contains 500 mg of Ampicillin, and the order is for 1.5 grams (which is 1500 mg). Therefore, you will need 3 vials of Ampicillin (1500 mg ÷ 500 mg/vial = 3 vials). Step 3: Calculate the total volume of Ampicillin solution.
Each vial contains 10 mL of Ampicillin solution, and you need 3 vials.
Therefore, the total volume of Ampicillin solution is 30 mL (3 vials × 10 mL/vial = 30 mL). Step 4: Calculate the total volume to be infused, including the Ampicillin solution. The total volume is 100 mL of Normal Saline + 30 mL of Ampicillin solution = 130 mL. Step 5: Calculate the infusion time in minutes.
The order is to infuse over 120 minutes.
Step 6: Calculate the flow rate in gtt/min.
Use the formula: Flow rate (gtt/min) = Total volume (mL) × Drop factor (gtt/mL) ÷ Infusion time (min) Plug in the values: Flow rate = 130 mL × 60 gtt/mL ÷ 120 min
Simplify: Flow rate = 7800 ÷ 120
Flow rate = 65 gtt/min
Therefore, the flow rate in gtt/min in which the IV fluid is to flow is 65 gtt/min.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today