A nurse is caring for a client at a follow-up visit who has been taking lithium therapy for bipolar disorder.
Which of the following findings should indicate to the nurse that the client is experiencing lithium toxicity?
Hypoglycemia.
Excess salivation.
Urinary retention.
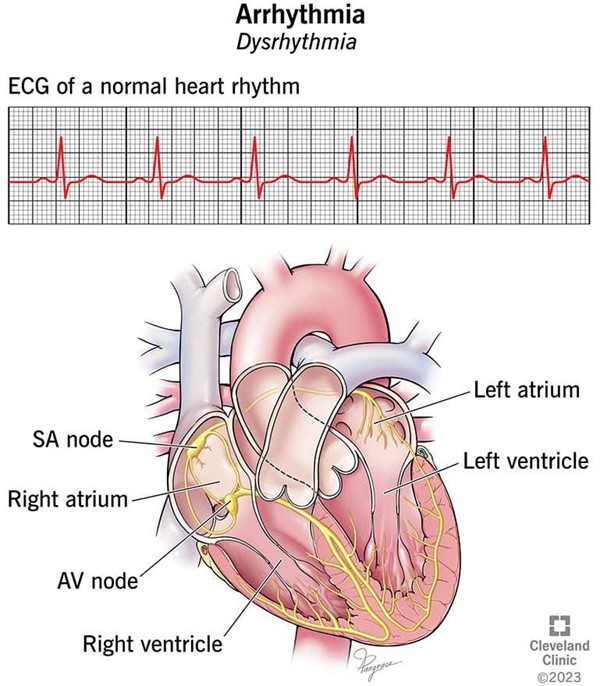
Dysrhythmia.
The Correct Answer is D
Dysrhythmia is an abnormal heart rhythm that can be a sign of severe lithium toxicity.
Lithium toxicity can occur when a person takes too much lithium, a mood- stabilizing medication used to treat bipolar disorder and major depressive disorder.
Choice A is wrong because hypoglycemia is not a symptom of lithium toxicity. Hypoglycemia is low blood sugar that can cause symptoms such as shakiness, sweating, hunger, and confusion.
Choice B is wrong because excess salivation is not a symptom of lithium toxicity. Excess salivation can be caused by various factors, such as infections, medications, or nerve damage.
Choice C is wrong because urinary retention is not a symptom of lithium toxicity. Urinary retention is the inability to empty the bladder completely, which can cause pain, discomfort, and infection. Lithium toxicity can actually cause increased urine output, not decreased.
Normal ranges for blood lithium levels are 0.6 to 1.2 mEq/L for maintenance therapy and 0.8 to 1.5 mEq/L for acute therapy. Levels above 1.5 mEq/L can cause mild to moderate toxicity, and levels above 2.0 mEq/L can cause severe toxicity. Levels above 3.0 mEq/L are considered a medical emergency.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
BMI 32.2.
A high body mass index (BMI) is a major risk factor for type 2 diabetes mellitus, as it indicates overweight or obesity.
Overweight or obesity can cause insulin resistance, which means the body cells do not respond well to insulin and cannot take up glucose from the blood. This leads to high blood sugar levels and diabetes.
Choice A is wrong because history of exercise-induced asthma is not a risk factor for type 2 diabetes mellitus.
Asthma is a respiratory condition that causes inflammation and narrowing of the airways, but it does not affect the metabolism of glucose or insulin.
Choice B is wrong because age 35 years is not a risk factor for type 2 diabetes mellitus.
Although the risk of diabetes increases with age, especially after 45 years, it can also occur in younger people.
Age alone is not enough to cause diabetes.
Choice C is wrong because history of mumps is not a risk factor for type 2 diabetes mellitus.
Mumps is a viral infection that affects the salivary glands, but it does not damage the pancreas or impair insulin production.
Some other risk factors for type 2 diabetes mellitus are family history, race or ethnicity, physical inactivity, prediabetes, gestational diabetes, polycystic ovarian syndrome, and smoking.
Correct Answer is D
Explanation
The nurse should determine if the client has prepared their advance directives, which are legal documents that specify the client’s wishes regarding medical care in case they become incapacitated. Advance directives can include a living will, a durable power of attorney for health care, or a do-not-resuscitate order. The nurse should respect the client’s autonomy and right to self-determination by asking about their advance directives and ensuring that they are documented and followed.
Choice A is wrong because the nurse should not delay the admission while the client fills out the facility’s advance directives form.
The client has the right to refuse or accept any treatment, including filling out an advance directives form.
The nurse should inform the client about the benefits of having advance directives, but should not coerce or pressure them to complete one.
Choice B is wrong because the nurse should not confirm with the client’s family that the consent form has been signed.
The consent form is a legal document that indicates that the client has given informed consent for the surgery, which means that they have received adequate information about the procedure, its risks and benefits, and alternative options.
The consent form should be signed by the client, unless they are a minor, mentally incompetent, or unable to communicate.
The nurse should verify that the consent form has been signed by the client or their legal representative before the surgery.
Choice C is wrong because the nurse should not explain to the client that signing the facility’s consent form means they cannot refuse care.
Signing the consent form does not waive the client’s right to withdraw consent at any time before or during the surgery.
The nurse should inform the client that they can change their mind and refuse care at any point, and that their decision will be respected and honored.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today