A nurse is caring for a client who has a new colostomy. The client tells the nurse, "I don't want anyone to
see me with this bag." Which of the following responses should the nurse make?
Many people have colostomies, and they live full lives
"Would it help to speak to someone else who has a colostomy?
Why don't you want people to see the colostomy bag?
The colostomy is probably only temporary
The Correct Answer is A
a. "Many people have colostomies and they live full lives."
Explanation:
The correct answer is a. "Many people have colostomies and they live full lives."
When a client expresses concerns or distress regarding their colostomy and not wanting others to see the colostomy bag, it is essential for the nurse to provide support and reassurance. Responding by acknowledging that many people live full lives with colostomies helps normalize the experience and offers hope to the client.
Option b, "Would it help to speak to someone else who has a colostomy?" may be a helpful suggestion, but it should not be the initial response. First, it is important to provide immediate reassurance and support to the client before exploring additional resources or contacts.
Option c, "Why don't you want people to see the colostomy bag?" may be seen as invasive and may put the client on the spot, potentially making them feel uncomfortable or defensive. It is important to create a safe and non-judgmental environment for the client.
Option d, "The colostomy is probably only temporary," assumes information about the client's specific situation that may not be accurate. It is important to avoid making assumptions about the duration or permanence of the colostomy unless the client has shared that information. Providing false reassurances can negatively impact the client's trust and emotional well-being.
By responding with the statement that many people live full lives with colostomies, the nurse offers support, normalizes the client's experience, and promotes a positive outlook for the client's future.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
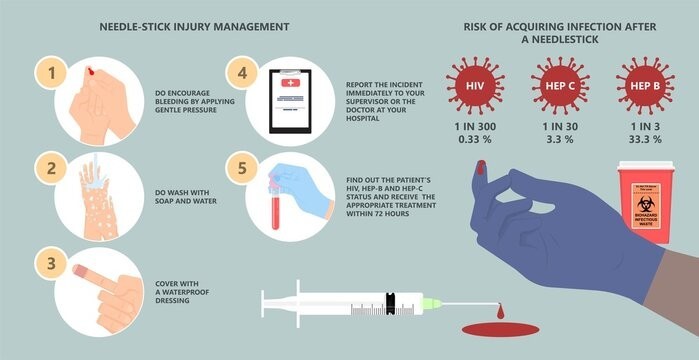
c. Dispose of the used needle immediately in a sharps container.
The nurse should dispose of the used needle immediately in a sharps container to reduce the risk of a needlestick injury. Sharps containers are specifically designed for the safe disposal of needles and other sharp objects. By placing the used needle directly into a sharps container, the nurse eliminates the need for handling or manipulating the needle further, reducing the risk of accidental needlestick injuries.
Explanation for the other options:
a. Place a cap holder securely on the used needle before disposal: Cap holders are not recommended for securing used needles before disposal. They may not provide adequate protection against needlestick injuries and can potentially increase the risk of accidental needlesticks when atempting to secure the cap holder.
b. Recap the needle for disposal later: Recapping the needle increases the risk of a needlestick injury. It is generally not recommended to recap needles after use, as it poses a greater risk of accidental puncture.
d. Detach the used needle and dispose of it promptly: Detaching the needle from the syringe before disposal is not recommended, as it increases the risk of a needlestick injury. It is safer to dispose of the needle and syringe as a unit in a sharps container to minimize the risk of accidental puncture.
Correct Answer is D
Explanation
The nurse should recommend that the client who has diminished breath sounds and paradoxical chest movement receive care first. This client is likely experiencing a tension pneumothorax, which is a life-threatening condition that requires immediate intervention.
Option a is incorrect because a client who has a head injury and whose pupils are fixed and dilated may have experienced brain death and may not be able to be resuscitated.
Option b is incorrect because a dislocated shoulder, while painful, is not immediately life-threatening. Option c is incorrect because a scalp laceration with intermittent bleeding can be managed with pressure and is not immediately life-threatening.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today