An nurse explains to new parents that their infant has developed Transient Tachypnea of the Newborn (TTN). The nurse understands that risk factors for TTN include which of the following?
Select one:
Preterm infant.
Female infant.
GBS status of mother.
Cesarean section.
The Correct Answer is D
Choice A Reason: Preterm infant. This is an incorrect answer that confuses TTN with another respiratory condition called respiratory distress syndrome (RDS). RDS is a serious condition where the newborn's lungs are immature and lack sufficient surfactant, which is a substance that reduces surface tension and prevents alveolar collapse. RDS can cause respiratory distress, hypoxia, acidosis, and organ failure. It is more common in preterm infants, especially those born before 37 weeks' gestation.
Choice B Reason: Female infant. This is an incorrect answer that has no evidence or rationale to support it. TTN does not have a gender preference or difference in incidence or severity.
Choice C Reason: GBS status of mother. This is an incorrect answer that relates to another respiratory complication called early-onset neonatal sepsis (EONS). EONS is a bacterial infection that occurs within 72 hours after birth, which can affect multiple organs and systems in the newborn. EONS can be caused by group B streptococcus (GBS), which is a common bacterium that colonizes in some women's vagina or rectum. GBS can be transmited to the newborn during delivery and cause pneumonia, meningitis, or septic shock.
Choice D Reason: Cesarean section. This is because cesarean section is a risk factor for TTN, which is a mild respiratory problem that results from delayed clearance of fetal lung fluid after birth. TTN causes rapid breathing, nasal flaring, grunting, and mild cyanosis. It usually resolves within 24 to 48 hours after birth. Cesarean section can increase the risk of TTN because it bypasses the normal process of labor, which helps squeeze out some of the fluid from the fetal lungs.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: Macrosomic newborn. This is a correct answer that describes a possible complication of post-term pregnancy. A macrosomic newborn is a newborn that weighs more than 4000 grams or 8 pounds 13 ounces at birth. It can occur in post-term pregnancies due to prolonged exposure to maternal glucose and insulin. It can increase the risk of birth injuries, shoulder dystocia, cesarean delivery, and hypoglycemia.
Choice B Reason: Intrauterine growth restriction (IUGR). This is a correct answer that indicates a potential problem of post-term pregnancy. IUGR is a condition where the fetal growth is slower than expected for gestational age. It can occur in post-term pregnancies due to placental insufficiency, aging, or calcification, which can impair nutrient and oxygen delivery to the fetus. It can increase the risk of fetal distress, hypoxia, acidosis, and stillbirth.
Choice C Reason: Umbilical cord prolapse. This is an incorrect answer that does not reflect a risk of post-term pregnancy, but rather a risk of other factors such as prematurity, low birth weight, breech presentation, multiple gestation, polyhydramnios, or artificial rupture of membranes.
Choice D Reason: Meconium Aspiration Syndrome (MAS). This is a correct answer that denotes a possible complication of post-term pregnancy. MAS occurs when fetal stool (meconium) enters into the lungs before or during birth, causing airway obstruction, inflammation, and infection. MAS usually affects term or post-term infants who experience fetal distress or hypoxia in utero. It can cause respiratory distress syndrome (RDS), persistent pulmonary hypertension (PPHN), or chronic lung disease (CLD).
Correct Answer is C
Explanation
Choice A Reason: 3-2-1-0-2. This is an incorrect answer that underestimates the number of pregnancies and overestimates the number of preterm births. The client has had four pregnancies, not three. She has had one preterm birth, not two.
Choice B Reason: 4-1-1-1-3. This is an incorrect answer that overestimates the number of living children. The client has two living children, not three.
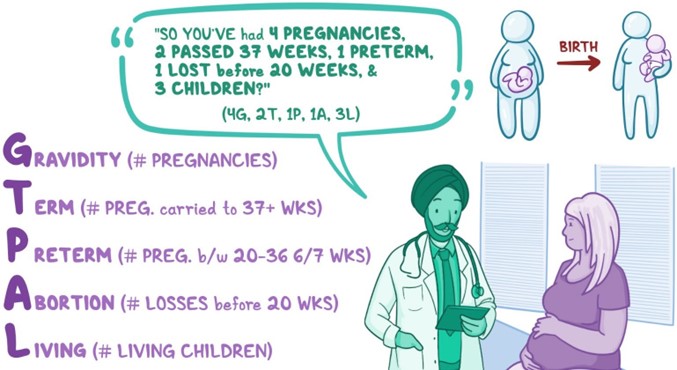
Choice C Reason 4-1-1-1-2. This is because the GTPAL method is a way of summarizing a woman's obstetric history using five numbers: G (gravida), T (term births), P (preterm births), A (abortions), and L (living children). Gravida is the number of pregnancies, regardless of outcome. Term births are deliveries after 37 weeks' gestation. Preterm births are deliveries between 20 and 37 weeks' gestation. Abortions are pregnancies that end before 20 weeks' gestation, either spontaneously or electively. Living children are the number of children who are alive at the time of assessment.
Choice D Reason: 4-1-2-0-3. This is an incorrect answer that overestimates the number of preterm births and living children, and underestimates the number of abortions. The client has had one preterm birth, not two. She has had one abortion, not zero. She has two living children, not three.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today